17 min read
May 31, 2026
AMH Test for PCOS and PMOS in Australia: What High AMH Means
Written by
Fertility2Family Team

Medically reviewed by
Evan Kurzyp, RN, BSN, Master of Nursing
AHPRA registration: NMW0002424871
A high AMH result can feel confusing, especially if PCOS or PMOS has been mentioned. AMH is useful, but it is only one blood test. It does not diagnose PMOS by itself, measure egg quality, confirm ovulation, or tell you whether you can get pregnant.
PMOS is the new name for PCOS. In adults, AMH can sometimes be used instead of pelvic ultrasound to support the ovarian morphology part of PMOS diagnosis. The result still needs to be read with your cycle pattern, androgen symptoms, blood tests, age and clinical history.
This guide explains what an AMH test means in Australia, when it may help with PCOS or PMOS assessment, what high AMH can and cannot tell you, how Medicare and private billing may work, and when to speak with your GP.
Quick Answers About AMH Tests for PCOS and PMOS
What is the AMH test for PCOS or PMOS?
The AMH test is a blood test that helps assess small follicle activity in the ovaries. In adult PMOS assessment, it may be used instead of ultrasound for the ovarian morphology part of diagnosis.
Does high AMH mean PMOS?
No. High AMH can support a PMOS diagnosis when other features are present, such as irregular cycles or signs of higher androgens. It does not prove PMOS on its own.
How much does an AMH test cost in Australia?
AMH test costs vary across Australia. Some providers advertise no out-of-pocket cost with a Medicare-valid referral, while others list private fees from about $50 to $100 or more. Ask the GP clinic and pathology provider before collection.
What is AMH and why does it matter in PMOS?
AMH stands for anti-Müllerian hormone. In adult women, it is made by granulosa cells around early ovarian follicles. These follicles are small and immature. They are not eggs being released that month.
An AMH result gives information about ovarian follicle activity. It does not measure egg quality, confirm ovulation, predict the exact time to pregnancy, or diagnose infertility. AMH is best read as ovarian response information, not a fertility score.
AMH matters in PMOS because many people with PMOS have more small follicles than expected for age. More small follicles can mean more AMH is produced. This is why AMH may help answer one diagnostic question: whether the ovaries show a follicle pattern that fits PMOS.
PMOS is the new name for the condition long known as PCOS. During the transition, Australian doctors, pathology forms and patient resources may still use PCOS. Fertility2Family’s main guide to what PMOS means in Australia explains the rename and why the condition is broader than ovarian cysts.
The 2023 guideline update on AMH
The 2023 International Guideline added AMH as an accepted alternative to ultrasound for defining polycystic ovarian morphology in adults. This is one of the main diagnostic changes since older PCOS criteria.
The guideline also sets limits. AMH should not be used as a single test for PMOS. AMH and ultrasound should not both be used for the same morphology question if doing so may increase overdiagnosis. AMH should not be used to diagnose PMOS in adolescents.
PMOS diagnosis still depends on a pattern. In adults, doctors usually assess ovulatory dysfunction, clinical or biochemical hyperandrogenism, and polycystic ovarian morphology. AMH may help with the morphology part, but it does not replace the rest of the assessment.
If irregular cycles and hyperandrogenism are already present, AMH or ultrasound may not be needed to make the diagnosis. If the diagnosis is unclear, AMH can help answer whether the ovarian follicle pattern fits the wider PMOS picture. For the full diagnostic pathway, read Fertility2Family’s guide to how PMOS is diagnosed in Australia.
AMH or ultrasound: which test matters more?
In adults, AMH may be used instead of ultrasound to answer the ovarian morphology part of PMOS diagnosis. That does not mean ultrasound is never useful. Ultrasound may still be needed if there is pelvic pain, abnormal bleeding, a suspected ovarian cyst, endometrial concerns, or another reason to look at the uterus and ovaries directly.
If AMH has already answered the morphology question, adding ultrasound only to prove the same point may increase overdiagnosis. If ultrasound is needed for another clinical reason, your GP can explain what the scan is looking for.

How AMH is tested and billed in Australia
AMH is tested with a standard blood draw. A GP, fertility specialist or gynaecologist may order it if it fits the clinical question.
Most people do not need to fast. AMH can usually be collected on any day of the menstrual cycle. If other hormone tests are being checked at the same time, your GP may give separate timing instructions.
Tell your GP if you use the contraceptive pill, hormonal contraception, fertility medicines, high-dose biotin, or if you are pregnant or breastfeeding. These details can affect timing or interpretation.
Australian pathology providers that may offer AMH testing include 4Cyte Pathology, Healius providers such as Laverty and QML, Australian Clinical Labs, Douglass Hanly Moir and Sullivan Nicolaides. Availability, collection sites, referral rules and billing can vary by state and provider.
How much does an AMH test cost in Australia?
AMH pricing in Australia is not the same everywhere. Some pathology providers advertise no out-of-pocket cost with a Medicare-valid referral. Other providers list AMH as privately billed, with prices often around $50 to $100 or more, depending on the provider and state.
This is why two Australian pages can appear to disagree: one provider may list AMH as privately billed, while another may advertise no out-of-pocket cost when referral requirements are met. Both can be true in their own setting.
The most useful question is not only “how much is the AMH test?” Ask whether the GP appointment has a gap fee, whether the pathology provider charges an AMH fee, whether collection costs apply, and whether your result will be reported in pmol/L with a lab reference range.
A common Australian situation is having AMH ordered on the same form as other blood tests. Some tests on that form may be bulk billed while AMH is billed separately. Ask before collection if cost matters.

Does Medicare cover the AMH test?
Medicare coverage and out-of-pocket billing for AMH depend on the provider, referral and clinical setting. This means there is no safe Australia-wide answer that applies to every person.
Some Australian providers advertise no out-of-pocket AMH testing when referral requirements are met. Others state that AMH is not covered by Medicare or attracts a private fee. Before testing, ask your GP and pathology provider whether AMH is bulk billed, privately billed, or partly covered in your situation.
When AMH may not be worth paying for yet
AMH may not be the first test to pay for if your main concern is missed periods, new acne, facial hair growth, heavy bleeding, pelvic pain, or a possible thyroid or prolactin problem. In those situations, a GP review and targeted blood tests may be more useful first.
It may also add little if PMOS is already clear from irregular ovulation and androgen excess, because AMH or ultrasound may not be needed to confirm the ovarian morphology feature. Ask what the AMH result would change before paying for the test.
AMH units in Australia: pmol/L vs ng/mL
Australian labs usually report AMH in pmol/L. Some overseas websites use ng/mL. This can make online comparison confusing.
A rough conversion is 1 ng/mL equals about 7.14 pmol/L. Even with conversion, use your own pathology report’s reference range rather than comparing your result with overseas tables.
Different labs can produce different AMH numbers from the same person. That does not always mean your body has changed. It may mean the test method or reference range is different.
AMH levels in PMOS: what is typical?
AMH is often higher in PMOS because more small follicles may be producing AMH. This can fit with the follicle pattern that used to be described as polycystic ovarian morphology.
Many Australian fertility resources describe a broad adult AMH range of about 7 to 30 pmol/L as common, while PMOS or PCOS may sit higher, sometimes around 35 to 50 pmol/L or above. These are examples, not diagnostic thresholds. Age, lab method, assay type and clinical context matter.
There is no single AMH number that diagnoses PMOS for every adult. Your result should be read against the lab’s reference range and your symptoms.
How to think about a low, normal or high AMH result
A low AMH result may suggest a lower follicle count for age, but it does not prove you cannot conceive. A typical-range AMH result may be reassuring for ovarian response, but it does not prove ovulation is regular. A high AMH result can fit with PMOS, but only when cycle pattern, androgen signs or blood tests also support the diagnosis.
The safest way to read AMH is by asking one question: what clinical decision will this result change? If it will not change diagnosis, fertility planning or IVF stimulation planning, repeating or chasing AMH numbers may add stress without changing care.

What if my AMH is high but I do not have PMOS symptoms?
High AMH without PMOS symptoms does not automatically mean PMOS. Some people have higher AMH because of age, individual variation, lab method or a higher follicle count without meeting diagnostic criteria.
PMOS is more likely when high AMH sits beside irregular or absent periods, signs of higher androgens, or androgen blood test changes. If your cycles are regular and you do not have androgen symptoms, your GP may interpret the result differently.
If your AMH is borderline or does not match your symptoms, ask what the result means for your age, which lab method was used, and whether any other tests are needed.
AMH and ovarian reserve are not the same question
The same AMH blood test can be used for two different questions. In PMOS assessment, AMH may help support the ovarian morphology part of diagnosis. In fertility planning, AMH is often used as one marker of ovarian reserve and likely response to stimulation medicines.
These are not the same question. A person with PMOS may have high AMH and still ovulate irregularly. A person with lower AMH may still ovulate and may still conceive.
AMH gives information about follicle number, not egg quality. Age remains one of the main factors linked with egg quality.
The common mistake is reading AMH as a fertility score. A high result does not mean pregnancy will be easy, and a lower result does not mean pregnancy is impossible. AMH is most useful when it answers a specific question, such as whether the ovarian follicle pattern supports PMOS diagnosis in an adult, or how the ovaries may respond to fertility medicines.
What AMH cannot tell you
AMH cannot tell you whether you ovulated this month, whether an egg was released, whether your egg quality is good, whether you will conceive naturally, or whether you have PMOS by itself. It also cannot replace a GP review when cycles are irregular, bleeding is absent, androgen symptoms are present, or pregnancy is not happening after a reasonable time.
AMH and fertility planning with PMOS
For people with PMOS who are trying to conceive, AMH is one part of the planning picture. It may help estimate ovarian response if treatment is needed, but it does not decide the whole plan.
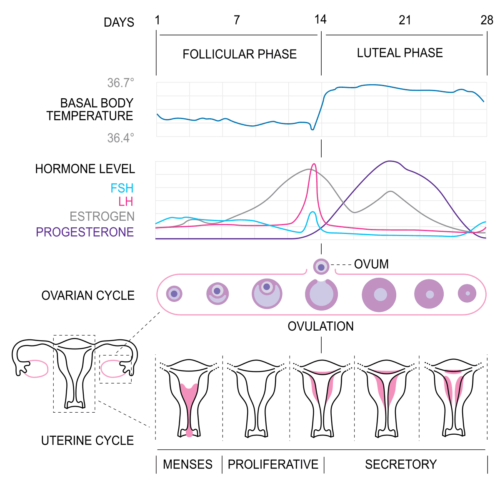
If cycles are irregular, the more practical question is often whether ovulation is happening and when. Ovulation test strips, cervical mucus tracking and basal body temperature can help collect cycle information to discuss with your GP, but they do not diagnose PMOS.
For women with irregular cycles trying to conceive, Fertility2Family’s PMOS fertility guide for Australia explains when to seek GP review, how ovulation tracking fits, and where fertility treatment may sit.
AMH and ovulation induction in PMOS
AMH level does not choose between letrozole, clomiphene or metformin for ovulation induction. Letrozole remains the recommended first-line option for anovulatory PMOS or PCOS when no other infertility factor is present, regardless of whether AMH is typical or high.
High AMH can suggest a stronger ovarian response if stimulation medicines are used, but the treatment decision is based on the full clinical picture, not AMH in isolation. Your specialist will consider age, cycle pattern, androgen results, semen analysis, tubal factors, ultrasound findings, previous response to medicines and safety risks.
AMH may influence how closely a cycle is monitored, especially if a stronger ovarian response is expected, but it should not be used alone to choose a medicine or dose.
For the full ovulation induction pathway, read Fertility2Family’s PMOS fertility guide for Australia.
AMH and IVF in PMOS
AMH is often used before IVF because it can help estimate how strongly the ovaries may respond to stimulation medicines. People with PMOS and high AMH may have a stronger ovarian response.
A stronger response can help with egg numbers, but it can also increase the risk of ovarian hyperstimulation syndrome. Fertility specialists use AMH, age, ultrasound findings and medical history to adjust medicine doses and monitoring.
AMH and antral follicle count are related but not identical. AMH is a blood marker. Antral follicle count is measured by ultrasound. Both can help describe ovarian response, but neither measures egg quality.
AMH and the contraceptive pill
Hormonal contraception can affect AMH interpretation in some people and can make other PMOS hormone tests harder to read. The combined oral contraceptive pill can also affect androgen testing.
Do not stop contraception only to change a blood test result unless your GP or specialist has advised this and you have a pregnancy prevention plan if needed.
AMH testing in adolescents
AMH should not be used to diagnose PMOS in adolescents. Normal puberty can overlap with PMOS-like patterns, including irregular cycles and changing hormone levels.
Adolescent assessment uses different rules and should be guided by a GP. In teenagers, diagnosis usually needs both ovulatory dysfunction and clinical or biochemical androgen excess, with other causes considered.
Limitations of AMH as a PMOS diagnostic test
AMH can also be affected by age, assay method, pregnancy, breastfeeding, ovarian surgery and some medical treatments. It must be interpreted in context, not read as a final answer by itself.
Significant weight change in either direction can temporarily shift AMH results, so timing testing during a period of weight stability may give a more useful baseline.
Pregnancy can suppress AMH substantially. Levels may take several months after birth or after breastfeeding ends to return toward baseline. If your result was taken during pregnancy, soon after birth or while breastfeeding, ask your GP whether retesting is worthwhile before drawing clinical conclusions.
The safest approach is to read AMH with your age, cycle pattern, androgen symptoms, blood tests, medicines, pregnancy history and the lab reference range.
When AMH testing is most useful
AMH testing is most useful in three situations: as part of the initial adult PMOS diagnostic workup when ultrasound is declined, inconclusive or not appropriate; as part of fertility planning when ovarian response is relevant; and as part of pre-IVF assessment when stimulation protocol planning is needed.
Outside these situations, AMH testing may add less and may not be worth the out-of-pocket cost. If your main concern is irregular cycles, the first step is often a GP review of ovulation pattern, androgen symptoms and metabolic health rather than AMH alone.
When to retest AMH or speak with your GP
AMH usually does not need frequent retesting for PMOS diagnosis. Once it has helped answer the morphology question, repeating it may not add much unless the result does not fit the clinical picture.
Retesting may be useful after a long gap, before fertility treatment, after ovarian surgery, after some cancer treatments, or if the first result was taken during pregnancy, breastfeeding or a time when interpretation was less reliable.
Ask your GP whether AMH testing is right for you if you have irregular cycles, possible PMOS, a previous PCOS diagnosis, fertility planning questions, or an AMH result that does not match your symptoms.
If you are under 35 and have been trying to conceive for 12 months, or 35 or older and have been trying for six months, book a GP review. Earlier review is reasonable if you have irregular cycles, known PMOS, repeated early losses, pelvic pain, endometriosis, thyroid disease, previous pelvic infection, or fertility treatment history.
Frequently Asked Questions About AMH Tests for PCOS and PMOS in Australia
Can AMH diagnose PMOS?
No. AMH cannot diagnose PMOS by itself. Under the 2023 International Guideline, AMH can support the ovarian morphology part of diagnosis in adults, but the full assessment still needs cycle, androgen and symptom context.
Does Medicare cover AMH testing in Australia?
It depends on the provider and referral setting. Some providers list AMH as privately billed, while others advertise no out-of-pocket AMH testing when referral requirements are met. Ask before collection.
Why do AMH test prices vary between Australian providers?
AMH prices vary because billing depends on the pathology provider, referral type, state, clinical setting and whether the test is privately billed or eligible for no out-of-pocket testing. Ask the provider before collection so you know the fee before the blood draw.
Does high AMH mean I am more fertile?
No. High AMH may suggest more small follicles or a stronger ovarian response, but it does not measure egg quality, prove ovulation or guarantee pregnancy. In PMOS, high AMH may sit beside irregular ovulation.
Does the pill affect AMH?
Hormonal contraception may affect AMH interpretation in some people and can affect other PMOS hormone tests. Tell your GP what contraception you use before testing.
Should teenagers have AMH testing for PMOS?
No. AMH is not recommended for diagnosing PMOS in adolescents. Teenage diagnosis uses different criteria because puberty can overlap with PMOS-like hormone and cycle patterns.
What to do with your AMH result
AMH can be useful when it answers the right question. Treat it as one part of the PMOS or fertility picture, not as a final answer on its own. If your result is high, low, borderline or confusing, take the report back to your GP and ask how it fits with your age, cycle pattern, symptoms, androgen results and pregnancy plans.
Last reviewed: May 20, 2026
Next scheduled review: May 2027
References
Fertility2Family publishes Australia-focused fertility education. Articles are written by our team and medically reviewed by Australian-registered health practitioners. We use Australian consumer medicine information, Australian clinical and public health guidance, and peer-reviewed research consistent with Australian care. We explain what the evidence suggests, what it cannot confirm, and when to see a GP or fertility specialist. Each article lists its author, medical reviewer, and review dates.
https://www.monash.edu/medicine/mchri/pcos/guideline
https://www.monash.edu/__data/assets/pdf_file/0003/3371133/PCOS-Guideline-Summary-2023.pdf
https://academic.oup.com/jcem/article/108/10/2447/7242360
https://www1.racgp.org.au/newsgp/clinical/pcos-officially-renamed-polyendocrine-metabolic-ov
https://www.jeanhailes.org.au/health-topics/pcos/
https://www.jeanhailes.org.au/articles/lets-talk-about-polycystic-ovary-syndrome/
https://www.askpcos.org/articles/pcos-diagnosis-and-hormone-levels/
https://www.4cyte.com.au/About/Services/AMH/
https://www.laverty.com.au/tests/anti-mullerian-hormone
https://antenatal.clinicallabs.com.au/patient/fertility/amh
https://www.clinpath.com.au/clinicians/tests-and-results/clinpath-tests/amh-fertility-test/
https://repromed.com.au/fertility-treatments/amh-blood-test/
https://www.ivf.com.au/planning-for-pregnancy/female-fertility/ovarian-reserve-amh-test
https://monashivf.com/services/early-intervention/amh-blood-test/
https://www.sydney.edu.au/news-opinion/news/2023/06/14/how-reliable-is-the-egg-time-blood-test.html
https://drdevora.com.au/anti-mullerian-hormone-test/
https://www.fertilitynorth.com.au/fertility-testing/amh-testing/