
Insulin resistance can sit behind PCOS or PMOS even when fasting glucose or HbA1c looks normal.
That is why some people have long cycles, acne, unwanted hair growth, energy dips or fertility concerns but are told their “blood sugar is fine”. Glucose can stay in range while the body makes more insulin to hold it there.
PCOS is now called PMOS, or polyendocrine metabolic ovarian syndrome. This guide explains how insulin resistance fits the condition, which tests Australian GPs may use, when OGTT, fasting insulin or HOMA-IR may help, what testing and medicines may cost, and where metformin, inositol, spironolactone, pregnancy planning and annual monitoring fit. For a broader explanation of the name change, see Fertility2Family’s guide to what PMOS means in Australia.
Quick Answers About PCOS and PMOS Insulin Resistance Australia
Is PMOS the same as insulin resistance?
No. PMOS is a hormone and metabolic syndrome. Insulin resistance is one common part of the pattern, but it is not the whole condition. Some people have strong metabolic features. Others have symptoms driven more by androgen excess, ovulation changes or genetics.
How do I know if I have insulin resistance with PCOS or PMOS?
You cannot know from symptoms alone. Long cycles, acne, hirsutism, energy dips, reactive hunger or weight changes may raise suspicion, but testing is needed. Your GP may check fasting glucose, HbA1c, lipids, blood pressure, fasting insulin, HOMA-IR or an OGTT.
Is metformin used for PCOS or PMOS insulin resistance in Australia?
Yes. Metformin is used in Australia for selected people with PCOS or PMOS, but use for PMOS itself is usually off label. It may help insulin resistance, cycle regularity and metabolic markers. Your GP should discuss dose, side effects, kidney function, B12 monitoring, pregnancy plans and cost.
Is PMOS the same as insulin resistance?
PMOS and insulin resistance are closely linked, but they are not the same thing.
PMOS is diagnosed from a wider pattern that may include irregular or absent ovulation, androgen excess and ovarian morphology or AMH findings, depending on age and context. Insulin resistance means body cells do not respond to insulin as efficiently as expected, so the pancreas may produce more insulin to keep blood glucose stable.
Diagnosis is covered separately in Fertility2Family’s PMOS diagnosis guide for Australia.
How insulin resistance can drive PMOS symptoms
Insulin helps move glucose from the bloodstream into cells. When cells respond poorly, the body may make more insulin. In PMOS, higher insulin can interact with the ovaries and adrenal pathways in ways that increase androgen activity.
One pathway involves theca cells in the ovaries. Higher insulin can make these cells more responsive to luteinising hormone, which can increase androgen production. Insulin can also reduce sex hormone binding globulin, often called SHBG. Lower SHBG means more free androgen may be active in the bloodstream.
Higher androgen activity can contribute to acne, unwanted facial or body hair, scalp hair thinning, irregular ovulation and long cycles. Insulin resistance can also disrupt signalling between the brain and ovaries, making ovulation less predictable.
The Rotterdam criteria and how these androgen and ovulation features are assessed are covered in Fertility2Family’s full PMOS Rotterdam criteria diagnostic guide for Australia.
Why insulin resistance can affect all body sizes
Insulin resistance is not limited to people in larger bodies. Lean PMOS is real, and some people have a typical BMI but still have high androgens, long cycles, acne, hirsutism, reactive hunger, energy dips or abnormal metabolic testing. Body size can affect risk, but it does not rule PMOS in or out.
PCOS insulin resistance tests in Australia
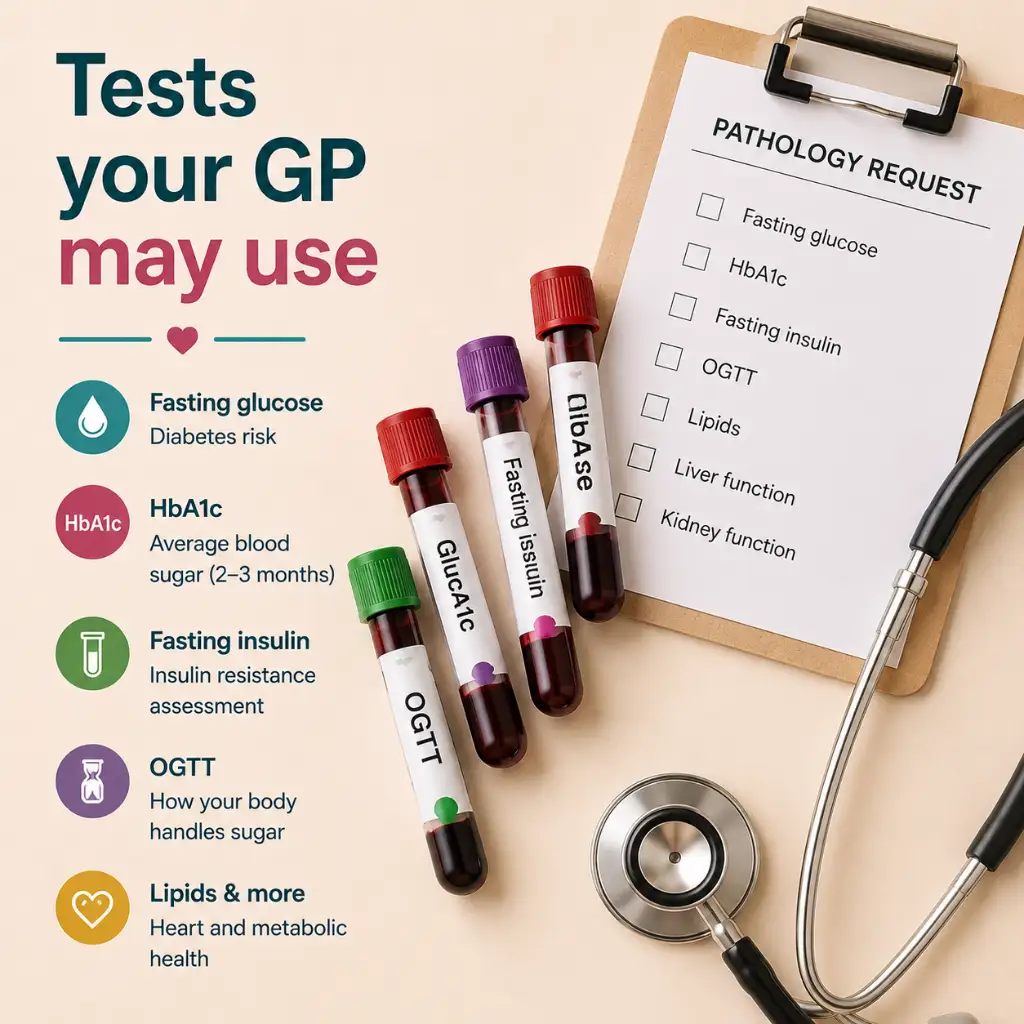
Your GP will usually start with tests that are accessible and linked to long-term risk. These may include fasting glucose, HbA1c, cholesterol, triglycerides, liver function, kidney function and blood pressure. Depending on your symptoms and goals, your GP may also request fasting insulin, HOMA-IR or an oral glucose tolerance test.
| Test | What it checks | How it helps in PCOS or PMOS | Australian cost context |
|---|---|---|---|
| Fasting glucose | Blood glucose after fasting | Useful for diabetes risk, but may miss early insulin resistance | Often bulk billed with a valid GP referral when Medicare-eligible |
| HbA1c | Average glucose over about three months | Useful and common, but less accurate than OGTT for some people with PCOS | Often bulk billed with a valid GP referral when clinically indicated |
| Fasting insulin | Insulin level after fasting | Can help when glucose is normal but insulin resistance is suspected | May be bulk billed by some providers or privately billed by others |
| HOMA-IR | A calculation using fasting glucose and fasting insulin | Can support interpretation, but cut-offs vary between labs and studies | Usually calculated from glucose and insulin results, not collected as a separate blood sample |
| OGTT | Glucose response after a 75 g glucose drink | The 2023 PCOS guideline describes OGTT as the most accurate glycaemic test | Often bulk billed when Medicare-eligible and GP-requested, but check before booking |
Fasting insulin, HOMA-IR, HbA1c and OGTT
Fasting insulin measures insulin after a fasting period, often around eight hours. It can help when glucose is normal but the body may be producing more insulin than expected. HOMA-IR uses fasting glucose and fasting insulin to estimate insulin resistance. Some clinicians and studies use cut-offs around 2.0 to 2.5, but there is no universal number for every lab, population or clinical situation.
Fasting glucose measures blood glucose at one point in time. HbA1c reflects average blood glucose over roughly three months. Both are useful, but they can miss some early or post-meal glucose problems in PCOS or PMOS.
An oral glucose tolerance test, or OGTT, checks how your body handles a measured glucose drink. The usual test involves a fasting blood sample, a 75 g glucose drink, and further blood samples after one hour and two hours. The 2023 international PCOS guideline describes OGTT as the most accurate test for glycaemic status in PCOS, regardless of BMI.
Before an OGTT, ask your GP or pathology provider how to prepare. Many collection centres require a booking because the test takes about two hours. Instructions may include fasting overnight, staying at the collection centre during the test, drinking water only, and following specific advice about food, caffeine, smoking, medicines and activity. Do not change medicines or diet for testing unless your doctor or pathology provider tells you to.
Where to get an OGTT or fasting insulin test in Australia
Common pathology providers include 4Cyte Pathology, Australian Clinical Labs and Healius brands such as Laverty Pathology in NSW and ACT, QML Pathology in Queensland, Dorevitch Pathology in Victoria and TML Pathology in Tasmania. Hobart readers may also see Hobart Pathology, Launceston Pathology or North West Pathology.
Billing differs by provider and test. Ask whether your OGTT, fasting insulin and related blood tests are bulk billed before you attend.
Metformin for PCOS and PMOS insulin resistance in Australia
Metformin is an insulin-sensitising medicine. It reduces glucose production by the liver and improves how the body responds to insulin. In PMOS, it may be used to support metabolic markers, cycle regularity and insulin resistance in selected people.
In Australia, metformin is PBS-listed for diabetes indications. Use for PMOS itself is usually off label, so your doctor should explain the reason, expected benefit, cost and follow-up plan. Metformin may be prescribed as immediate-release or extended-release tablets. Extended-release metformin is sometimes used when stomach side effects limit tolerance.
PBS-listed brand examples include Diaformin, Formet, Glucobete, Diabex XR and other generic metformin brands, but availability and pricing can change. Some products may cost below the PBS maximum, while others may have a brand premium. Ask your pharmacist whether a lower-cost equivalent is available.
Metformin is often started at a low dose to reduce stomach side effects. Some people start with 500 mg daily, then increase slowly if tolerated. Common clinical dosing for PMOS may sit around 1,500 mg to 2,000 mg daily, but your GP decides the dose based on your health, tolerance, kidney function, other medicines and goals.
Common side effects include nausea, loose stools and stomach discomfort. Extended-release metformin or taking it with food may improve tolerance. Long-term use can reduce vitamin B12 in some people, so ask your GP whether monitoring is needed.
If fertility is the main goal, metformin may have a role for some people, but ovulation induction medicines may be more effective when anovulatory infertility is present. Fertility treatment options are covered in Fertility2Family’s PMOS fertility and pregnancy guide.

Inositol and insulin resistance
Inositol is a naturally occurring compound involved in insulin signalling. The two forms most discussed in PMOS are myo-inositol and d-chiro-inositol. Many PMOS supplements use a 40:1 ratio, often described as 4 g myo-inositol with 100 mg d-chiro-inositol per day, split across two doses.
Inositol is available over the counter in Australia. It may suit some people who want a non-prescription option or cannot tolerate metformin. The evidence is less certain than for metformin, and supplement quality, strength and cost can vary.
For dosing context, product quality and safety notes, read Fertility2Family’s inositol for PCOS and PMOS guide. For the difference between forms, see Fertility2Family’s myo-inositol and d-chiro-inositol comparison guide. For a broader overview of supplements studied in PMOS, see Fertility2Family’s PMOS supplements guide for Australia.

Metformin vs inositol for PCOS insulin resistance
| Option | Main role | Cost context |
|---|---|---|
| Metformin | Prescription insulin-sensitising medicine with stronger clinical use for metabolic features | PBS-listed for diabetes indications. Patient charge varies by product, brand and eligibility |
| Inositol | Over-the-counter supplement involved in insulin signalling, with less certain evidence | Usually privately purchased, with cost varying by brand, dose and pack size |
| Both together | Sometimes discussed when metabolic symptoms persist or one option is not enough | May involve both prescription and supplement costs, so discuss with your GP |
What does PCOS insulin resistance care cost in Australia?
Costs vary by provider, referral, Medicare eligibility, billing policy, medicine brand and pharmacy. With a GP referral, many routine pathology tests are bulk billed. If a test is not bulk billed, the provider should explain any out-of-pocket cost before testing.
| Care item | Australian cost context | What to ask |
|---|---|---|
| Routine blood tests and OGTT | Often bulk billed when Medicare-eligible and GP-requested | Ask whether any requested tests attract a fee |
| Fasting insulin | Billing varies more than routine glucose testing | Ask whether it is bulk billed or privately billed |
| Metformin | PBS-listed for diabetes indications. In 2026, the general PBS maximum is $25 and concession is $7.70, but some products may cost less or have brand premiums | Ask whether your script is PBS-subsidised and whether IR or XR is being used |
| Spironolactone | PBS-listed. Patient charge varies by strength and brand, and some brands may have a premium | Ask the pharmacist whether a lower-cost equivalent is available |
| Dietitian support | Private fees vary. Some people with eligible chronic condition plans may access Medicare-subsidised allied health visits | Ask your GP about care-plan eligibility and ask the dietitian about gap fees |
Lifestyle, diet and weight without restriction
Lifestyle care for PMOS should not mean blame, restriction or being told to lose weight without proper assessment. The goal is to support insulin sensitivity, energy, sleep, cycle information and long-term health.
Resistance training can help because muscle is a major site of glucose use. Walking, cycling, swimming and other aerobic movement also support glucose control and cardiovascular health.
There is no single PMOS diet. A useful food pattern usually focuses on regular meals, enough protein, high-fibre carbohydrates, lower-GI choices where practical, vegetables, legumes, fruit, nuts, seeds, olive oil, dairy or calcium alternatives, and enough total food to avoid rebound hunger. For detailed food examples, read Fertility2Family’s PCOS diet Australia guide and PMOS eating patterns guide for Australian women.
GLP-1 medicines and SGLT-2 inhibitors
GLP-1 and dual GIP/GLP-1 medicines, including semaglutide, liraglutide, dulaglutide and tirzepatide, are discussed more often in PMOS because they can affect appetite, weight and cardiometabolic markers. In Australia, their approvals relate to type 2 diabetes and/or chronic weight management, not PMOS itself.
They are not first-line PMOS care for everyone and are not used during pregnancy. SGLT-2 inhibitors are also diabetes medicines, not routine PMOS treatment, but may be considered in selected people with type 2 diabetes or other indications under medical guidance.
Spironolactone and androgen symptoms in PMOS
Insulin resistance can increase androgen production in PMOS. Treating insulin resistance may reduce androgen activity over time, which is one reason metformin, movement, sleep and food-pattern changes can sometimes improve acne or unwanted hair growth.
Some people need more targeted androgen management. Spironolactone is an anti-androgen medicine used for persistent acne or hirsutism in PMOS when other measures are not enough.
Spironolactone with PCOS or PMOS does not treat insulin resistance directly. It works on the symptom side of androgen excess by blocking androgen effects on skin and hair follicles. It may be used alongside metabolic treatment, not instead of it.
Spironolactone is generally used off label for PMOS. It is not suitable during pregnancy, and reliable contraception is needed when pregnancy is possible. Side effects can include dizziness, breast tenderness, menstrual changes and potassium changes. Your GP, dermatologist or endocrinologist can assess whether it is suitable and whether blood monitoring is needed.
If androgen symptoms changed suddenly, became severe, or came with voice deepening, rapid scalp hair loss or marked body changes, seek prompt medical review rather than assuming PMOS is the cause.
Long-term risks and pregnancy
PMOS is linked with higher risk of impaired glucose tolerance, type 2 diabetes, abnormal cholesterol, high blood pressure, cardiovascular disease and fatty liver. Individual risk varies, which is why regular metabolic review matters.
If you are pregnant or planning pregnancy with PMOS, ask your GP, obstetrician or fertility specialist about early glucose screening. Some people may be offered earlier testing around 12 to 16 weeks, followed by the usual pregnancy OGTT at 24 to 28 weeks if needed.
Metformin may be continued or stopped in pregnancy depending on why it was prescribed and your clinical context. Ask the prescribing doctor what applies to you. For the full PMOS pregnancy and gestational diabetes pathway, read Fertility2Family’s getting pregnant with PMOS guide for Australia.
When to ask for referral
Your GP may manage insulin resistance in PMOS if results are mild, symptoms are stable and treatment is straightforward. Referral may be useful if glucose results are abnormal, insulin resistance is severe, medicines are not tolerated, androgen symptoms are difficult to control, pregnancy planning is complex, or another endocrine condition needs to be ruled out.
An endocrinologist may help with insulin resistance, diabetes risk, high androgens, metformin intolerance, GLP-1 or SGLT-2 suitability, or unusual hormone results. A gynaecologist or fertility specialist may be more appropriate when irregular ovulation, bleeding, pelvic symptoms or fertility treatment is the main concern. Regional patients can ask about telehealth, shared-care or public outpatient options.
Monitoring frequency for metabolic health
Metabolic monitoring should be planned, not left until symptoms appear. Many people benefit from at least yearly review with their GP, though timing depends on age, results, pregnancy plans, medicines and family history.
A useful PMOS review may include blood pressure, glucose or HbA1c, lipids, liver function, cycle pattern, skin or hair symptoms, mental health, sleep apnoea symptoms and medicine review. The 2023 guideline recommends assessing glycaemic status at diagnosis and repeating testing over time. OGTT may be considered where accuracy matters, especially before pregnancy or fertility treatment.
What to ask your GP
Ask whether your PCOS or PMOS review should include fasting glucose, HbA1c, lipids, blood pressure, liver function, fasting insulin, HOMA-IR or an OGTT. If pregnancy or fertility treatment is planned, ask whether OGTT is preferred over HbA1c alone.
Before pathology, ask whether fasting insulin is included, whether you need to fast, whether there may be an out-of-pocket cost, and when your GP will review the result. If medicine is discussed, ask whether it is on label or off label, what side effects to watch for, and when to review.
Frequently Asked Questions About PCOS Insulin Resistance Australia
How do I know if I have insulin resistance with PCOS?
You cannot confirm insulin resistance from symptoms alone. Long cycles, acne, hirsutism, energy dips, reactive hunger, weight changes or a family history of diabetes may raise suspicion, but your GP needs to interpret symptoms with blood pressure, glucose, HbA1c, lipids and sometimes fasting insulin, HOMA-IR or OGTT results.
What blood test shows insulin resistance in PCOS?
No single blood test proves every case of insulin resistance. Fasting glucose and HbA1c check glucose control. Fasting insulin and HOMA-IR can suggest higher insulin demand. OGTT is the most accurate glycaemic test recommended in the 2023 PCOS guideline, especially when pregnancy planning or fertility treatment matters.
Can you have PCOS insulin resistance with normal glucose?
Yes. Blood glucose can stay normal while the body produces more insulin to keep it there. This is why some people with PCOS or PMOS have normal fasting glucose but still have raised fasting insulin, abnormal OGTT results or symptoms that fit insulin resistance.
Is metformin better than inositol for PCOS insulin resistance?
They are different. Metformin has stronger clinical use history for metabolic features, but it can cause gastrointestinal side effects and needs medical prescribing. Inositol is available over the counter and may be easier to tolerate, but evidence is less certain and product quality varies.
Does spironolactone help insulin resistance in PCOS?
No. Spironolactone is used for androgen-related symptoms such as hirsutism or acne. It does not treat insulin resistance directly. In PMOS, it may be used alongside metabolic care when androgen symptoms remain distressing.
Can lean people with PCOS or PMOS have insulin resistance?
Yes. Lean PMOS can still involve insulin resistance, high insulin, androgen symptoms and ovulation changes. Body size alone should not decide whether metabolic testing is considered.
Next Steps in Australia
If you have PMOS and have never had metabolic testing, book a GP review and bring your cycle history, symptoms, medicines, contraception details, pregnancy plans, family history of diabetes, previous pathology and any home tracking notes.
Ask which tests are needed now, whether an OGTT is appropriate, whether fasting insulin or HOMA-IR would add useful information, and when results should be reviewed.
If you are trying to conceive, combine medical care with practical cycle tracking. Ovulation test strips, basal body temperature, cervical mucus notes and pregnancy test strips can help you collect useful information, but they should support GP or fertility review rather than replace it.
Last reviewed: May 20, 2026
Next scheduled review: May 2027
References
Fertility2Family publishes Australia-focused fertility education. Articles are written by our team and medically reviewed by Australian-registered health practitioners. We use Australian consumer medicine information, Australian clinical and public health guidance, and peer-reviewed research consistent with Australian care. We explain what the evidence suggests, what it cannot confirm, and when to see a GP or fertility specialist. Each article lists its author, medical reviewer, and review dates.
https://www1.racgp.org.au/newsgp/clinical/pcos-officially-renamed-polyendocrine-metabolic-ov
https://academic.oup.com/jcem/article/108/10/2447/7242360
https://www.monash.edu/__data/assets/pdf_file/0003/3379521/Evidence-Based-Guidelines-2023.pdf
PCOS to PMOS Australia: Symptoms, Diagnosis, Ovulation and Fertility
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/polycystic-ovarian-syndrome-pcos
https://dietitiansaustralia.org.au/health-advice/polycystic-ovary-syndrome-pcos
Polycystic Ovary Syndrome: what diabetes educators need to know
https://australianprescriber.tg.org.au/articles/pharmacological-management-of-polycystic-ovary-syndrome.html
https://australianprescriber.tg.org.au/articles/gestational-diabetes-update-on-screening-diagnosis-and-maternal-management.html
https://www.racgp.org.au/afp/2012/june/oral-glucose-tolerance-testing
https://www.racgp.org.au/afp/2012/october/polycystic-ovary-syndrome
https://www.racgp.org.au/afp/2012/march/skin-androgen
https://www.tga.gov.au/safety/safety-monitoring-and-information/safety-alerts/new-diabetes-and-weight-loss-medicines
https://www.pbs.gov.au/info/healthpro/explanatory-notes/front/fee
https://www.pbs.gov.au/medicine/item/13976N-2430X
https://www.pbs.gov.au/medicine/item/2339d-2340e
https://www.healthdirect.gov.au/paying-for-diagnostic-testing
https://www.servicesaustralia.gov.au/bulk-billing
https://www.servicesaustralia.gov.au/pbs-safety-net-thresholds
https://www.laverty.com.au/pre-test-collection-information/glucose-tolerance-test-gtt
https://www.clinicallabs.com.au/patient/test-instructions/glucose-tolerance-test-gtt
https://www.4cyte.com.au/Patients/Before/pt_instructions_gtt.pdf
https://www.healius.com.au/our-businesses
https://www.thewomens.org.au/images/uploads/fact-sheets/METFORMIN-2020.pdf
https://www.endocrinesociety.org.au/position-statement-metformin.asp
https://www.healthdirect.gov.au/polycystic-ovarian-syndrome-pcos