
13 min read
Dec 4, 2025
Fertile Window: How Long Does Ovulation Last?
Written by
Fertility2Family Team

Medically reviewed by
Evan Kurzyp, RN (AHPRA), BSN, Master of Nursing
Understanding your fertile window can help you time intercourse for the best chance of pregnancy. The fertile window is the cluster of days when sperm and egg can meet. Sperm may live for up to five days in the reproductive tract, while the egg usually lives for 12 to 24 hours after it is released. That is why the days before ovulation matter as much as the day itself. You can estimate your window with cycle tracking, ovulation predictor kits and body signs. If your cycles vary a lot or you have symptoms such as pelvic pain, it is sensible to see your GP. This guide uses Australian care pathways and plain language so you can plan with confidence and know when to seek support.
Quick Answers About the Fertile Window
How long does ovulation last
The egg is usually viable for 12 to 24 hours after release. Your fertile window is wider because sperm can survive in fertile cervical mucus for up to five days.
When am I most fertile
The highest chance of conception is the day before ovulation and on the ovulation day itself. The two days before ovulation also carry a solid chance.
What is the fastest way to find my fertile days
Use an LH ovulation predictor kit to detect the surge, watch for clear stretchy cervical mucus, and confirm a small basal temperature rise after ovulation. Test at a consistent time and follow the kit instructions.
What the fertile window is and how ovulation works
Your fertile window includes the five days before ovulation and the ovulation day. This timing reflects how long sperm may stay active in fertile mucus and how brief egg survival is once released. If sperm are present in the fallopian tube when the egg arrives, conception can occur. You might know that the best time to have intercourse if you are trying to conceive is when you ovulate, but the lead up matters as well. The egg is usually available for only a day. Sperm arriving in the days before ovulation can wait for the egg in the fallopian tube.
Your cycle length and the day you ovulate can vary from cycle to cycle. Some people ovulate earlier or later than the mid cycle day. Research shows ovulation can happen between day 6 and day 21 depending on the person and the cycle. Learning the pattern of your own cycle helps you time sex with less guesswork and stress.
Right Time For Sex: When is my fertile window?
What affects the timing of ovulation
The brain ovaries and uterus work together each cycle. The pituitary gland releases follicle stimulating hormone to grow follicles, rising oestrogen thickens the uterine lining and signals a spike in luteinising hormone known as the LH surge. That LH surge triggers ovulation. After ovulation the follicle becomes the corpus luteum and makes progesterone to prepare the lining for implantation.
Many factors can shift when you ovulate. Common influences include age, cycle length and natural variability. Health and lifestyle can also play a role. Sudden weight change, low body fat, heavy exercise, poor sleep, acute illness, shift work and major stress may alter timing. Medical conditions such as polycystic ovary syndrome, endometriosis, thyroid disorders and raised prolactin can disrupt ovulation or make it unpredictable. Some medicines can affect cycles. If your periods have become scarce, very frequent or highly irregular, see your GP for assessment. Early review can help confirm whether ovulation is occurring and guide treatment where needed.
How to track ovulation at home
There are several ways to predict ovulation from home. The calendar method uses past cycle lengths to estimate the next fertile window. It can be a starting point but is less reliable if cycles vary because it assumes consistent timing. Many people prefer to track body signs and hormones for a clearer picture.
Watching your fertility hormones can be helpful. There is a Luteinising hormone surge 24 to 36 hours before ovulation, and peak concentrations are found at 10 to 12 hours before ovulation. Oestrogen rises in the three to five days leading to ovulation. As these hormones drive ovulation, their changes are a useful guide.
Ovulation predictor kits detect the LH surge in urine. Fertility2Family’s ovulation predictor kits are designed to show when LH is high so you can plan intercourse around likely ovulation. Test daily around your expected window and read the result at the time stated on the packet. A positive usually means ovulation is likely within the next day or so. People with polycystic ovary syndrome can sometimes see frequent positives because baseline LH can be higher. If your kits are confusing for several cycles, speak with your GP.
Basal body temperature can also help. Your basal body temperatures may dip slightly just before ovulation and then lift after ovulation when progesterone rises. Before ovulation, basal temperature often sits around 36.1 to 36.4 degrees Celsius. About 24 hours after ovulation, it rises to around 36.4 to 37 degrees. A sensitive thermometer such as Fertility2Family’s basal thermometer can detect the small shift. Temperature confirms that ovulation has already happened, so combine it with other signs to predict the days ahead.
The cervix and its mucus change with hormones. Early in the cycle mucus is thicker and may look creamy or cloudy. As oestrogen rises it becomes clear, wet and stretchy like raw egg white. This change supports sperm survival and movement. Noticing this transition can help you identify approaching fertility. The cervix often sits higher, feels softer and the opening is a little wider near ovulation. If you are comfortable, you can check this gently with clean hands and track what feels normal for you. More detail on these signs is outlined by the research on fertility awareness methods and general guides such as cervix position changes.
What ovulation and pregnancy tests involve
Ovulation predictor kits are urine tests that compare the test line to a control. When the test line is as dark or darker than the control, that indicates an LH surge. Digital kits show a clear symbol. For reliable tracking, begin testing a few days before the date you expect an LH rise based on your usual cycle or previous kits. Test at a consistent time each day and avoid excess fluids beforehand. Read results within the time window on the leaflet. Certain medicines, fertility injections that contain hCG, and some hormonal conditions can affect results. Fertility2Family’s blog explains how to time testing across short and long cycles.
Home pregnancy tests detect human chorionic gonadotropin in urine. Levels usually rise after implantation, which tends to occur six to twelve days after ovulation. The most reliable time to test is from the day your period is late. Testing earlier can give a negative even if you are pregnant because hCG may not yet be high enough to detect. If you test early and get a negative, test again after a day or two if your period does not arrive. If you get a faint positive, repeat after forty eight hours to check for a stronger result. Always follow the packet directions and time the reading carefully.
Planning intercourse across the fertile window
Timing sex in the two days before ovulation and on the day can lift your chance of conception. Studies of people with regular cycles suggest the chance of pregnancy may range from about 0.4 to 7 percent five days before ovulation, 8 to 17 percent four days before, 8 to 23 percent three days before, 13 to 29 percent two days before, 21 to 34 percent the day before, 8 to 33 percent on the day and around 0.8 to 11 percent the day after. These figures vary with age, cycle patterns and overall health. They reflect the biology of sperm survival and egg lifespan rather than a guarantee for any one cycle.
Many couples aim for intercourse every one to two days across the fertile window, starting a few days before the expected LH surge or the first day of fertile type mucus. This pattern keeps sperm available in the reproductive tract while keeping sex comfortable and sustainable. Choose a simple water based lubricant labelled sperm friendly if you use one. Some standard lubricants can reduce sperm movement. If tracking is stressful, regular intercourse through the middle of the cycle is a practical approach.

What happens to your body when you ovulate?
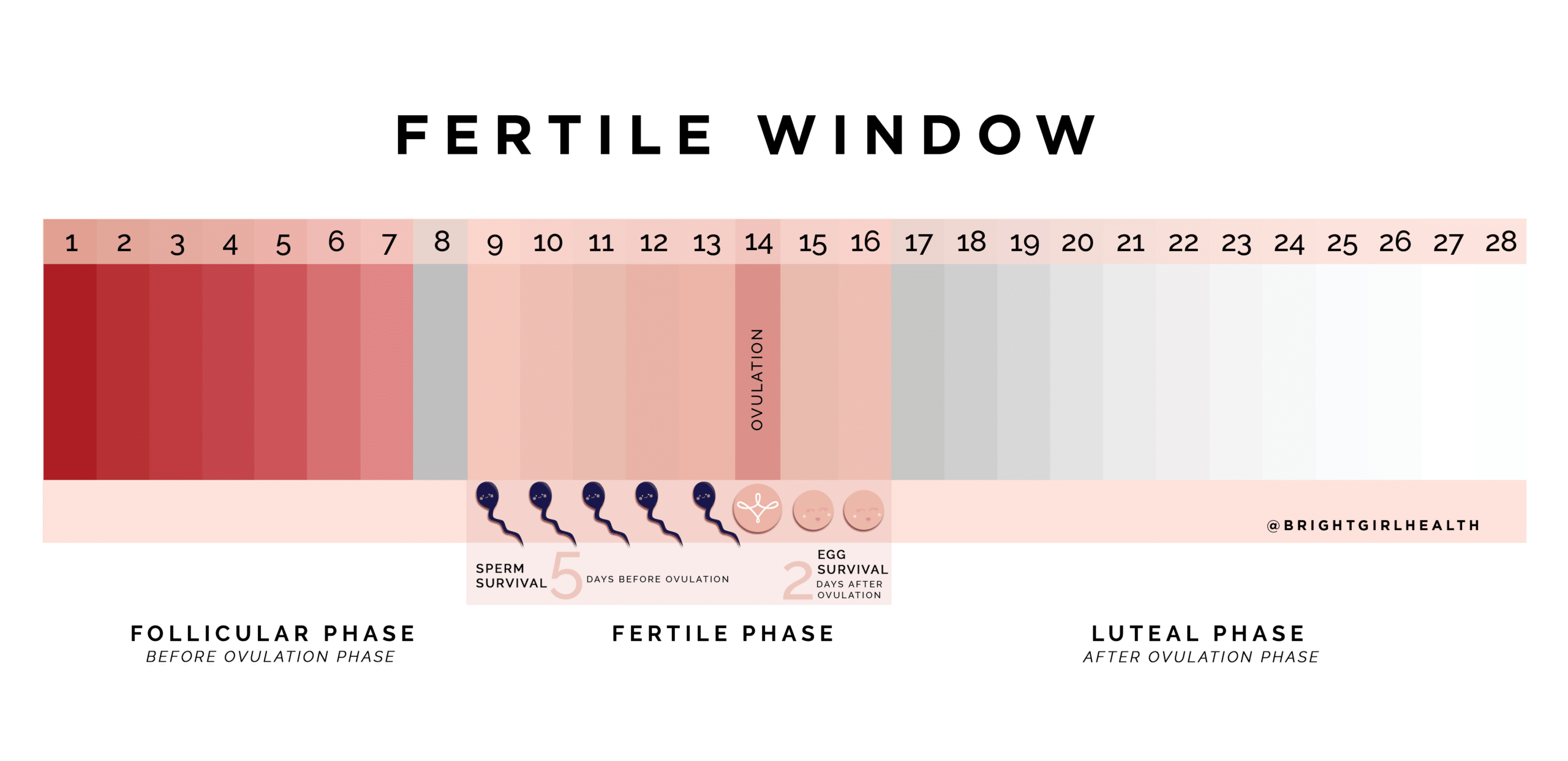
Image courtesy of
Guide by Demi Spaccavento.
Practical lifestyle strategies to support regular ovulation
Small changes at home can support hormone balance and cycle regularity. Aim for steady sleep and wake times and get seven to nine hours of sleep. Gentle routines such as guided breathing, meditation or yoga can help manage stress and may blunt cortisol spikes that influence cycle hormones. If work or care demands are heavy, brief pauses to stand, stretch and breathe can settle the nervous system.
Choose regular meals that include whole grains, vegetables, fruit, legumes, nuts, seeds and lean proteins. Including omega 3 sources such as oily fish and walnuts can help with general inflammation and may support reproductive health. The Australian Dietary Guidelines provide an accessible framework for balanced eating across the week.
Move your body most days with activities you enjoy such as brisk walking, swimming, cycling or yoga. Moderate exercise supports a healthy weight and insulin sensitivity, both linked with ovulation. Very intense training without enough rest can disrupt cycles in some people, so build in recovery. If you are planning notable changes to your diet or training, a chat with your GP or a dietitian can help you tailor a plan to your health needs.
When to see a GP or specialist in Australia
See your GP if you have been trying for twelve months without pregnancy if you are under 35. If you are 35 or older, book a review after six months. Seek care sooner at any age if your cycles are very irregular, you have severe pelvic pain or heavy bleeding, known conditions such as polycystic ovary syndrome or endometriosis, a history of pelvic infection or pregnancy loss, or concerns about thyroid or prolactin issues. If you are not having periods, do not wait to be seen.
Your GP will usually take a detailed history, review cycle tracking, discuss timing of intercourse and assess lifestyle factors. They may arrange blood tests to check ovulation with a progesterone level about seven days after suspected ovulation, thyroid function, prolactin and iron. Some people are offered an AMH test to estimate ovarian reserve, though it does not predict the exact chance of pregnancy in a given cycle. A pelvic ultrasound can assess ovaries and the uterus. Screening for sexually transmitted infections may be advised. Your GP can refer to a RANZCOG specialist or fertility clinic if needed. Medicare rebates apply to many assessments and your GP can explain costs and options.
Optimising ovulation predictor kits and combining methods
Fertility peaks during the surge of luteinising hormone. Fertility2Family’s Ovulation Predictor Kits detect this spike. For consistent results, test at the same time each day and follow packet directions on when to begin and how to read the lines. Fluid intake, shift work, stress and some medicines can alter hormone timing and give unexpected patterns. If you receive inconsistent results, keep notes for several cycles and discuss them with your GP if you remain unsure.
Combining methods improves accuracy. Use OPKs to predict the surge, watch for clear stretchy mucus in the days before the positive, then look for a small basal temperature rise in the day or two after. This sequence lines up with the hormone pattern that drives ovulation. Keep a simple daily record of what you notice in one place. After a few cycles you may see a pattern that makes planning easier and calmer.
Frequently Asked Questions About the Fertile Window Australia
Can I get pregnant outside the fertile window
It is unlikely because the egg lives for about a day and sperm need fertile mucus to survive for long. Pregnancy is still possible if ovulation timing was earlier or later than expected.
Does an LH surge guarantee I will ovulate
An LH surge usually precedes ovulation, but some conditions like polycystic ovary syndrome can produce false positives. Tracking temperature after the surge helps confirm that ovulation occurred.
Do I need to have sex on the exact ovulation day
Not necessarily. The best chances are the day before and the day of ovulation. Sex every one to two days in the fertile window covers the key days without pressure to pinpoint the exact hour.
Can breastfeeding or stopping hormonal contraception affect ovulation timing
Yes. Breastfeeding can suppress ovulation for a time. After stopping hormonal contraception, cycles may take weeks to months to settle. Track signs and see your GP if cycles have not returned after a few months.
My OPKs are always positive or never positive. What should I do
Always positive can reflect high baseline LH which is seen in some people with polycystic ovary syndrome. Never positive may mean a short surge or mistimed testing. Keep records and see your GP for assessment.
Are there medical checks I can request before trying
Yes. A preconception GP visit can cover immunisation, folate and iodine, rubella and varicella status, STI screening, thyroid function where indicated and a plan for any ongoing conditions. This helps set up healthy cycles and pregnancy.
A final word for Australian readers
Most people benefit from a simple plan. Learn the signs that ovulation is approaching, choose one or two tools you will actually use and give yourself a few cycles to see a pattern. Many find that an LH kit plus a quick daily note on cervical mucus gives enough clarity. Others like the reassurance of confirming ovulation with a small temperature rise the next morning. If tracking becomes a source of worry, keep sex regular through the middle of the cycle and focus on sleep, food you enjoy and movement that feels good. When questions keep coming up, bring your records to your GP and ask for a preconception check. If you want at home tools, Fertility2Family’s ovulation predictor kits and basal thermometers are designed to fit into everyday life. The blog explains common questions about timing, kit use and cycle changes so you can plan your next steps with clear, practical information.
References
https://www.healthdirect.gov.au/ovulation
https://www.healthdirect.gov.au/fertility
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/ovulation
https://ranzcog.edu.au/patients/fertility-and-reproductive-health
https://www.jeanhailes.org.au/health-a-z/menstruation/ovulation
https://www.fpnsw.org.au/education/health-professionals/clinical-resources/fertility-awareness
https://www.qld.gov.au/health/staying-healthy/sexual-health/fertility
https://www.health.nsw.gov.au/kidsfamilies/MCFhealth/Pages/preconception-health.aspx


