16 min read
May 22, 2026
PCOS Symptoms, Now Called PMOS: Signs, Cycles, Skin and Fertility in Australia
Written by
Fertility2Family Team

Medically reviewed by
Evan Kurzyp, RN, BSN, Master of Nursing
AHPRA registration: NMW0002424871
PMOS symptoms can include irregular or absent periods, acne, excess facial or body hair, scalp hair thinning, delayed ovulation, reduced fertility, insulin resistance, weight changes, mood symptoms and sleep problems. PMOS is the new name for PCOS, or polycystic ovary syndrome. The symptoms have not changed, but the new name better reflects that the condition can affect endocrine, metabolic and ovarian health.
One symptom does not prove PMOS. A pattern of symptoms can suggest it is worth seeing a GP, especially when cycle changes, androgen signs or metabolic risk appear together. In Australia, diagnosis usually starts with cycle history, symptom review, blood tests and sometimes ultrasound. This guide explains the main PMOS symptoms, what they can mean, what they cannot prove, and when to seek medical advice.
Quick Answers About PMOS Symptoms Australia
What are the most common PMOS symptoms?
The most common PMOS symptoms are irregular or absent periods, acne, oily skin, excess facial or body hair, scalp hair thinning, delayed ovulation, difficulty conceiving, weight changes and signs of insulin resistance. Some people also notice anxiety, low mood, sleep problems or fatigue.
Is PMOS the same as PCOS?
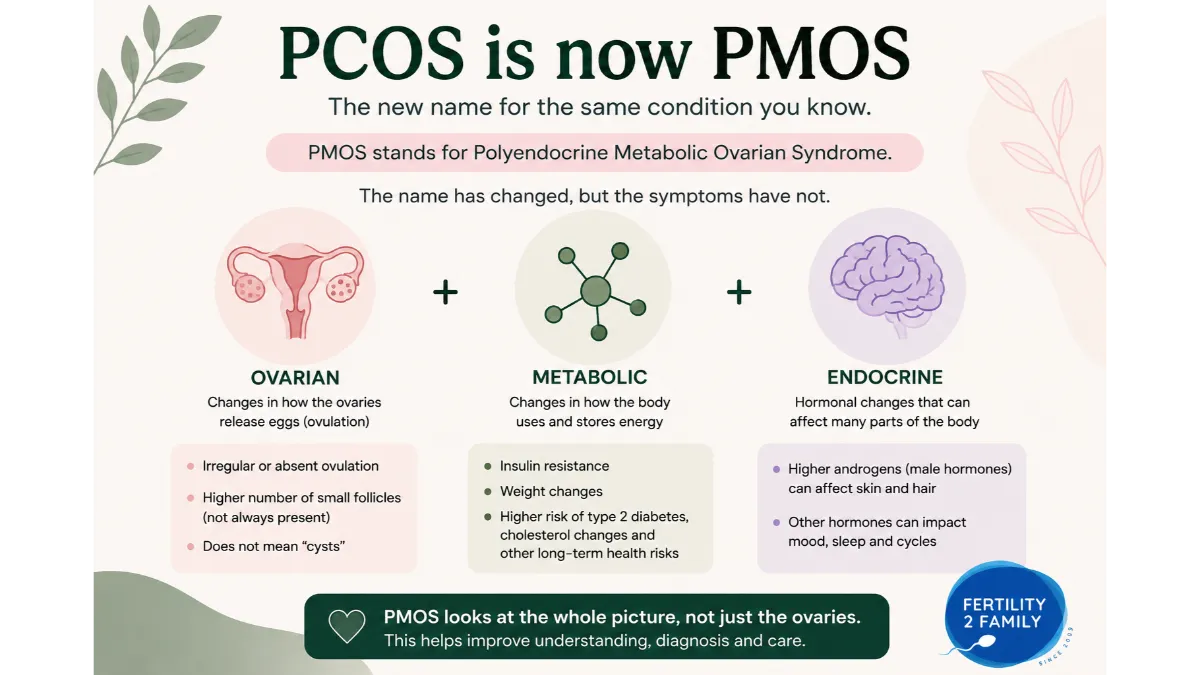
Yes. PMOS is the new name for the same condition previously called PCOS. PMOS stands for polyendocrine metabolic ovarian syndrome. During the transition, Australian health resources may use both PCOS and PMOS together.
Can I have PMOS symptoms with a normal ultrasound?
Yes. A normal ultrasound does not always rule out PCOS, now PMOS. Symptoms, cycle pattern, androgen signs and blood tests also matter. Ultrasound can help in some adult diagnostic pathways, but it should not be treated as the only answer.
PMOS Symptoms Guide Australia
Cycle symptoms: PMOS can cause periods to come late, stop for months, or arrive unpredictably. Long cycles can mean ovulation is delayed or not happening every cycle.
Skin and hair symptoms: Acne, oily skin, excess facial or body hair and scalp hair thinning can occur when androgen levels are higher or when hair follicles are more sensitive to androgens.
Metabolic symptoms: PMOS can be linked with insulin resistance, higher diabetes risk, cholesterol changes, weight changes, cravings or fatigue. These symptoms can occur across body sizes.
Fertility symptoms: PMOS can make trying to conceive harder when ovulation is irregular or absent. It does not mean pregnancy is impossible.
Symptoms that need medical review: periods absent for months, sudden heavy bleeding, rapidly worsening hair growth, severe acne, pelvic pain, symptoms of high blood sugar, or difficulty conceiving should be discussed with a GP.
PCOS Is Now PMOS: Why the Name Changed
PCOS has been renamed PMOS, which stands for polyendocrine metabolic ovarian syndrome. The new name was recommended in May 2026 after an Australian-led global consensus process published in The Lancet.
The rename was led by Professor Helena Teede from Monash University and involved international patient, public and health professional input. The change moves attention away from “cysts” and towards the endocrine, metabolic and ovarian features that can affect health across the lifespan.
This matters for symptoms because PMOS is not only an ovary or fertility condition. Symptoms can involve cycles, skin, hair, ovulation, insulin resistance, sleep, mood and long term metabolic health.
In plain language, PMOS symptoms are not only symptoms “on the ovary”. They can show up in the menstrual cycle, skin, hair, metabolism, mood, sleep and fertility, which is why the new name better fits the condition.
If you are trying to work out whether an ultrasound finding is PCO, PCOS or PMOS, read Fertility2Family’s diagnostic guide to PCO vs PCOS and PMOS diagnosis in Australia. This page stays focused on symptoms and when to seek help.
Irregular Periods and Missed Periods with PMOS
Irregular periods are one of the main PMOS symptoms. A cycle may be longer than expected, unpredictable, absent for months, or hard to track.
Long cycles often mean ovulation is delayed. In some cycles, ovulation may not happen. This can make fertile-window timing harder and can also make pregnancy testing confusing.
Irregular bleeding can have other causes. Thyroid changes, prolactin changes, pregnancy, perimenopause, some medicines, stress, weight change, eating disorders and hormonal contraception can also affect bleeding. A GP can help separate PMOS from other causes.
A practical example is a 42-day cycle with acne and new facial hair. That pattern does not confirm PMOS, but it is enough to record cycle dates and book a GP review. A single late period after illness or travel may be less concerning, but repeated long cycles should not be ignored.
Long gaps between periods should be discussed with a GP. Regular shedding of the uterine lining matters for endometrial health, and your GP can advise whether bleeding pattern, medicines or further tests need review.
Ovulation Symptoms and Fertility Signs
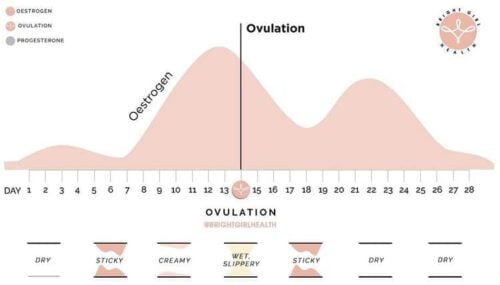
PMOS can affect fertility mainly by making ovulation irregular or absent. If ovulation happens late, the fertile window also shifts later.
You may still notice egg-white cervical mucus, pelvic twinges, breast tenderness or libido changes. These signs can suggest hormone changes, but they do not prove ovulation occurred.
Ovulation tests can help some people with regular enough cycles. In PMOS, baseline luteinising hormone may be higher or surge patterns may be harder to read. A repeated positive or confusing ovulation-test pattern should be checked against cycle dates, cervical mucus, temperature tracking or GP-arranged progesterone blood testing.
Fertility2Family’s guide to fertile cervical mucus without ovulation explains why one fertile sign may not tell the whole story. A future PMOS ovulation-tracking guide can cover LH testing patterns in more depth.
Acne, Oily Skin and PMOS
Acne and oily skin can be PMOS symptoms, especially when they appear with irregular periods, excess facial or body hair, or scalp hair thinning.
Androgens can increase oil production in the skin. This may contribute to acne on the face, jawline, chest or back. Acne alone does not diagnose PMOS, because acne can also occur from skincare products, medicines, stress, hormonal contraception changes or other hormone patterns.
See a GP if acne is persistent, painful, scarring, sudden in adulthood, or appearing with new cycle changes or hair growth. A GP can check whether androgen testing, contraception review, skin treatment or referral is needed.
Facial Hair, Body Hair and Hirsutism
Excess facial or body hair can occur with PMOS. The medical term is hirsutism. It usually refers to thicker, darker hair in areas such as the upper lip, chin, jaw, chest, abdomen or back.
Hirsutism can happen when androgen levels are higher or when hair follicles are more sensitive to androgens. It can also run in families or vary by ancestry.
New, fast or severe hair growth should be reviewed promptly. Rapid change, voice deepening, marked muscle changes or sudden severe acne may need earlier medical assessment because other androgen-related conditions can look similar.
Scalp Hair Thinning and Hair Shedding
Scalp hair thinning can be a PMOS symptom, but it should not be assumed to be PMOS without checking other causes.
Androgen-related hair thinning often appears around the part line, crown or front of the scalp. Hair shedding can also occur after illness, stress, low iron, thyroid changes, rapid weight change, childbirth, some medicines or restrictive eating.
Ask your GP about blood tests if hair shedding is new, heavy, persistent or paired with irregular cycles. Iron studies, thyroid function, androgen testing and other checks may help guide the next step.
Weight Changes, Cravings and Insulin Resistance
PMOS can be linked with insulin resistance, but insulin resistance can occur at any body size. The PMOS rename helps move care away from assuming the condition only matters in people in larger bodies.
Some people notice weight gain, strong cravings, fatigue after meals, difficulty with appetite regulation, or a family history of type 2 diabetes. These signs can suggest metabolic strain, but they do not prove insulin resistance by themselves.
Your GP may check glucose, HbA1c, cholesterol, blood pressure and sometimes an oral glucose tolerance test. These tests help guide care and reduce the chance of missing metabolic risk.
Do not use PMOS symptoms as a reason for blame. Body size alone cannot confirm or exclude PMOS. A lower-BMI person can still have irregular ovulation, androgen symptoms or insulin resistance. A larger-bodied person still deserves careful assessment without assumptions.
PMOS can also be linked with longer term metabolic risks, including type 2 diabetes risk, cholesterol changes, high blood pressure, fatty liver risk and sleep apnoea risk in some people. These are not symptoms you can confirm from appearance. They are reasons to ask your GP which checks are suitable for you.
Mood, Anxiety, Sleep and Fatigue
PMOS can affect mental wellbeing and quality of life. Some people experience anxiety, low mood, poor sleep, body image distress, fatigue or stress related to symptoms.
These symptoms are real, but they can have many causes. Iron deficiency, thyroid changes, depression, anxiety disorders, sleep apnoea, shift work, stress, medicines and pregnancy can all overlap with PMOS symptoms.
See a GP if mood, sleep or fatigue symptoms affect daily life, work, relationships or safety. If you feel at risk of harming yourself, seek urgent help through emergency services, Lifeline or a local crisis service.
PMOS Symptoms at Different Life Stages
Symptoms can look different across adolescence, adult onset, TTC, pregnancy planning, postpartum years and perimenopause.
In teenagers, irregular cycles and acne can be part of normal puberty. This is why diagnosis in adolescents is handled carefully. Labelling too early can cause harm, but repeated or severe symptoms still deserve review.
When trying to conceive, the main symptom issue is often irregular ovulation. Cycles may be long, ovulation tests may be confusing, and pregnancy tests may be taken too early if ovulation happened later than expected.
In the 40s, PMOS symptoms can overlap with perimenopause. Cycle changes, skin changes, sleep changes and weight changes may need a broader review rather than assuming one cause.
PMOS Symptoms Checklist
Use this as a prompt for your GP appointment, not as a self-diagnosis tool.
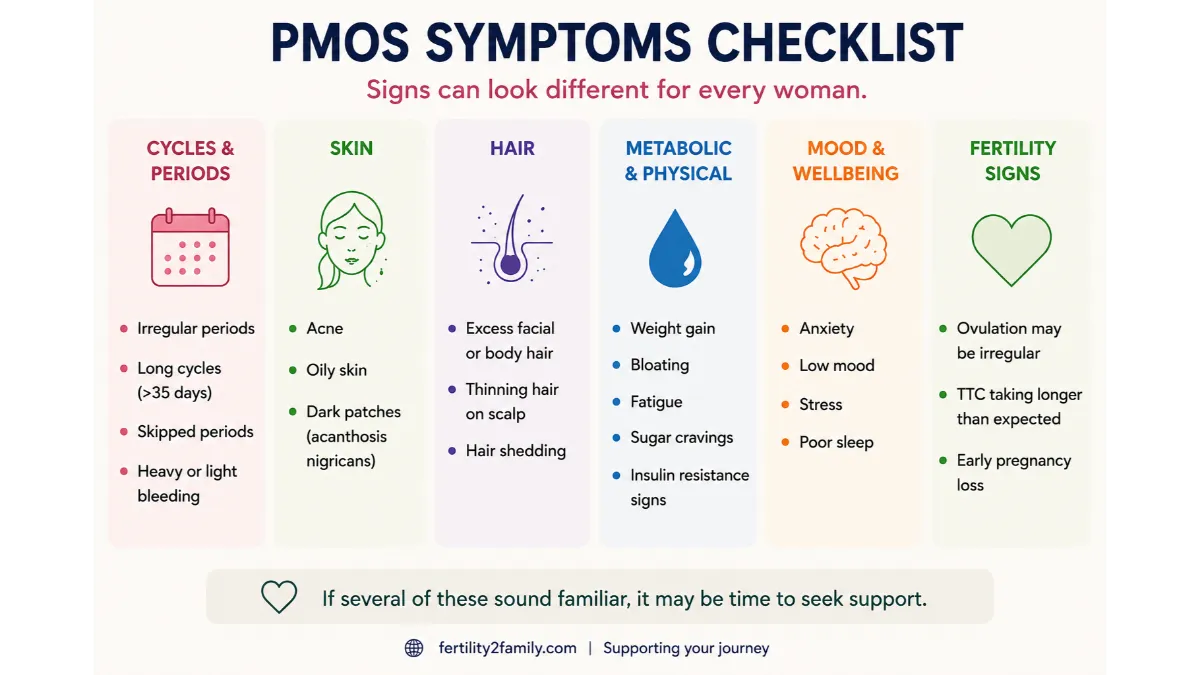
Cycle pattern: cycles longer than 35 days, missed periods, unpredictable bleeding or absent periods for months.
Skin and hair: persistent acne, oily skin, excess facial or body hair, scalp hair thinning or new hair shedding.
Fertility signs: difficulty finding ovulation, repeated confusing ovulation tests, long cycles while trying to conceive, or no clear temperature shift after suspected ovulation.
Metabolic signs: strong cravings, fatigue after meals, weight changes, family history of diabetes, high cholesterol or past gestational diabetes.
Wellbeing signs: anxiety, low mood, sleep problems, body image distress or fatigue that affects daily life.
When to book: repeated symptoms, symptoms across more than one group, or symptoms affecting fertility, skin, mental wellbeing or metabolic health are reasonable reasons to book a GP appointment.
PMOS Symptoms vs Other Conditions
PMOS symptoms can overlap with other conditions. That is why diagnosis should not be made from a checklist alone.
Endometriosis can cause pelvic pain, painful periods, pain with sex and fertility problems. Thyroid disease can affect periods, energy, weight, mood and hair shedding. High prolactin can affect periods and sometimes cause nipple discharge. Perimenopause can affect cycles, sleep, mood and bleeding patterns.
Some people have more than one condition. For example, PMOS and endometriosis can both affect fertility, but they do it in different ways. A GP can decide whether blood tests, ultrasound, pelvic pain assessment or referral is needed.
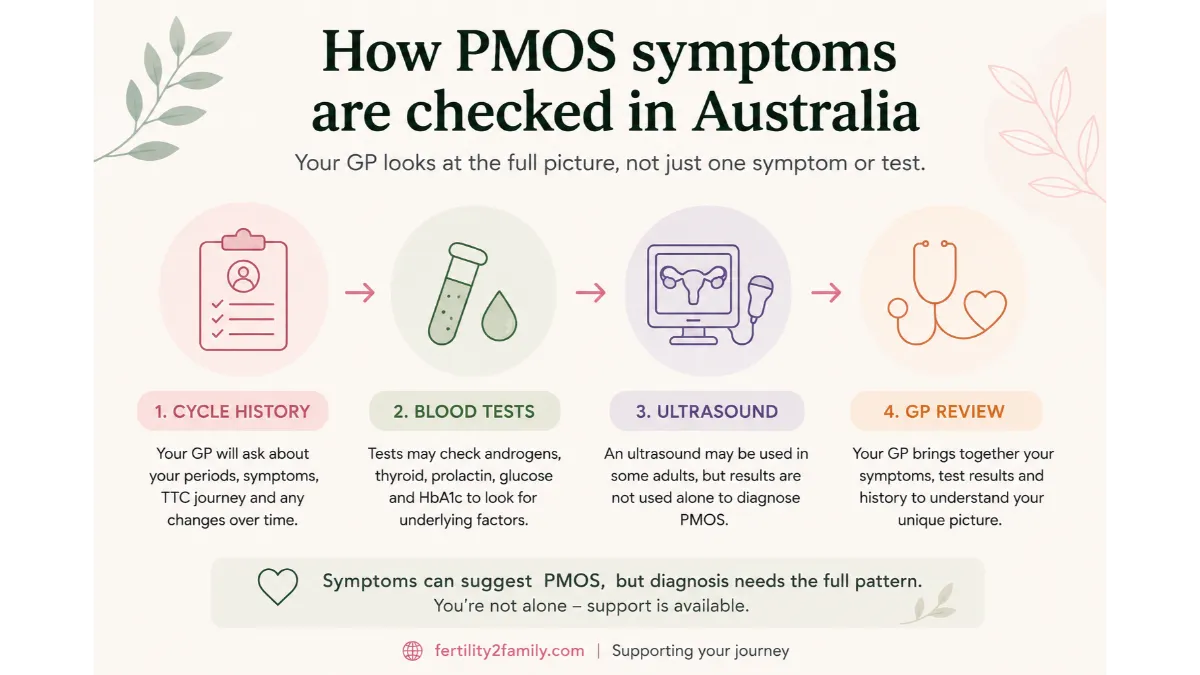
How PMOS Symptoms Are Checked in Australia
In Australia, the first step is usually a GP appointment. Your GP can review your cycle history, symptoms, medicines, contraception history, family history and TTC timeline.
Blood tests may check androgens, sex hormone binding globulin, thyroid function, prolactin, glucose, HbA1c, cholesterol and other markers depending on your situation. A progesterone blood test may help confirm whether ovulation likely occurred.
Ultrasound may be used in some adults, but it is not always needed and should not be read alone. If you want the diagnostic pathway in more detail, use Fertility2Family’s guide to PMOS diagnosis, ultrasound and blood tests in Australia.
If your main question is supplements, read the guide to PCOS supplements in Australia, now PMOS. If your main question is dose and timing, read the guide to taking inositol for PCOS, now PMOS.
When to See a GP About PMOS Symptoms
See a GP if your periods are often more than 35 days apart, absent for months, very heavy, very painful, or unpredictable. Also seek advice for persistent acne, new facial or body hair, scalp hair thinning, difficulty conceiving, symptoms of insulin resistance, or mood symptoms affecting daily life.
If you are trying to conceive, book a fertility review after 12 months if you are under 35, or after 6 months if you are 35 or older. Earlier review is reasonable if your cycles are irregular, absent or hard to track.
Seek earlier care if symptoms change quickly. Fast worsening hair growth, sudden severe acne, fainting, severe pelvic pain, very heavy bleeding, or symptoms of high blood sugar need medical review.
Before the appointment, record your cycle dates, symptoms, medicines, supplements, contraception use, ovulation-test patterns and pregnancy-test timing. This gives your GP a clearer pattern to work from.
Frequently Asked Questions About PMOS Symptoms Australia
What are the first signs of PMOS?
Early signs can include irregular periods, missed periods, acne, oily skin, excess facial or body hair, scalp hair thinning, difficulty tracking ovulation, weight changes or signs of insulin resistance. One sign alone does not confirm PMOS. A repeated pattern is the reason to speak with a GP.
Can PMOS symptoms come and go?
Yes. Symptoms can change with age, contraception use, weight change, stress, sleep, pregnancy, breastfeeding, medicines and metabolic health. Symptoms may improve for a time and return later. A GP can help decide whether the change fits PMOS or another cause.
Can you have PMOS without weight gain?
Yes. PMOS can occur across body sizes. Weight gain can happen, but it is not required for PMOS. Insulin resistance, irregular ovulation and androgen symptoms can occur in people with a lower BMI, so body size alone should not decide whether testing is needed.
Can you have PMOS with regular periods?
It is possible, but regular periods make the pattern less obvious. Some people with regular bleeding may still have androgen symptoms or metabolic features. If symptoms are persistent or you are unsure whether you ovulate, discuss this with your GP.
Does acne mean I have PMOS?
No. Acne alone does not diagnose PMOS. Acne can have many causes, including skincare products, stress, medicines, contraception changes and other hormone patterns. Acne is more suggestive of PMOS when it appears with irregular cycles, excess hair growth, scalp thinning or blood-test changes.
Does facial hair mean I have PMOS?
Not always. Facial hair can be genetic or related to normal variation. It is more concerning when it is new, worsening, thick, dark, or paired with irregular periods, acne or scalp hair thinning. Rapid change should be reviewed earlier.
Can PMOS cause anxiety or low mood?
PMOS can be linked with anxiety, low mood and reduced quality of life. These symptoms can also have other causes. If mood symptoms affect your daily life, sleep, work, relationships or safety, see a GP or mental health professional.
Are PMOS and endometriosis symptoms the same?
No. They can overlap, especially around fertility concerns, but they are different conditions. Endometriosis is more often linked with pelvic pain, painful periods and pain with sex. PMOS is more often linked with irregular ovulation, androgen symptoms and metabolic risk. Some people can have both.
Can PMOS affect pregnancy chances?
PMOS can affect pregnancy chances when ovulation is irregular or absent. Many people with PMOS still conceive, sometimes naturally and sometimes with medical support. Fertility also depends on age, sperm factors, tubal health, endometriosis, timing and general health.
Should I use ovulation tests if I have PMOS symptoms?
Ovulation tests can help if your cycles are regular enough to predict when to test. With PMOS, LH patterns can be harder to interpret. If tests are repeatedly positive, always negative or do not match your cycle signs, use them with cycle tracking and ask your GP about progesterone testing.
Next Steps in Australia
If PMOS symptoms fit your pattern, book a GP appointment with your cycle dates, symptom notes, medicines and TTC timeline. If you are tracking while waiting for review, Fertility2Family’s ovulation test strips may help when cycles are regular enough to choose a testing window, and pregnancy tests can be used from the right time after suspected ovulation. Fertility2Family is Australian-owned since 2009 and offers discreet packaging with tracked Australia-wide delivery, but irregular cycles, confusing ovulation tests or suspected PMOS should be reviewed with a GP.
Last reviewed: May 2026. Next scheduled review: May 2027.
References
Fertility2Family publishes Australia-focused fertility education. Articles are written by our team and medically reviewed by Australian-registered health practitioners. We use Australian consumer medicine information, Australian clinical and public health guidance, and peer-reviewed research consistent with Australian care. We explain what the evidence suggests, what it cannot confirm, and when to see a GP or fertility specialist. Each article lists its author, medical reviewer, and review dates.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00717-8/fulltext
https://www1.racgp.org.au/newsgp/clinical/pcos-officially-renamed-polyendocrine-metabolic-ov
https://www.endocrine.org/news-and-advocacy/news-room/2026/pcos-name-change
https://www.healthdirect.gov.au/polycystic-ovarian-syndrome-pcos
https://www.jeanhailes.org.au/health-topics/pcos/
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/polycystic-ovary-syndrome-pcos
https://www.monash.edu/medicine/sphpm/mchri/pcos/guideline
https://www.monash.edu/__data/assets/pdf_file/0003/3371133/PCOS-Guideline-Summary-2023.pdf
https://www.healthdirect.gov.au/insulin-resistance
https://www.healthdirect.gov.au/glucose-tolerance-test