17 min read
May 19, 2026
How Is PMOS Diagnosed in Australia? PCOS, PCO and Testing Explained
Written by
Fertility2Family Team

Medically reviewed by
Evan Kurzyp, RN, BSN, Master of Nursing
AHPRA registration: NMW0002424871
PMOS is the new name for PCOS, but the way the condition is diagnosed has not suddenly changed. In Australia, PMOS diagnosis usually starts with a GP review of your cycle pattern, androgen symptoms, blood tests and, when needed, pelvic ultrasound or AMH.
This guide explains how PMOS is diagnosed, what PCO means on an ultrasound report, why polycystic ovaries alone are not enough for diagnosis, and which tests your GP may use to rule out similar conditions. If you want the broader naming background first, start with our guide to what is PMOS in Australia.
Quick Answers About PMOS Diagnosis in Australia
How is PMOS diagnosed in Australia?
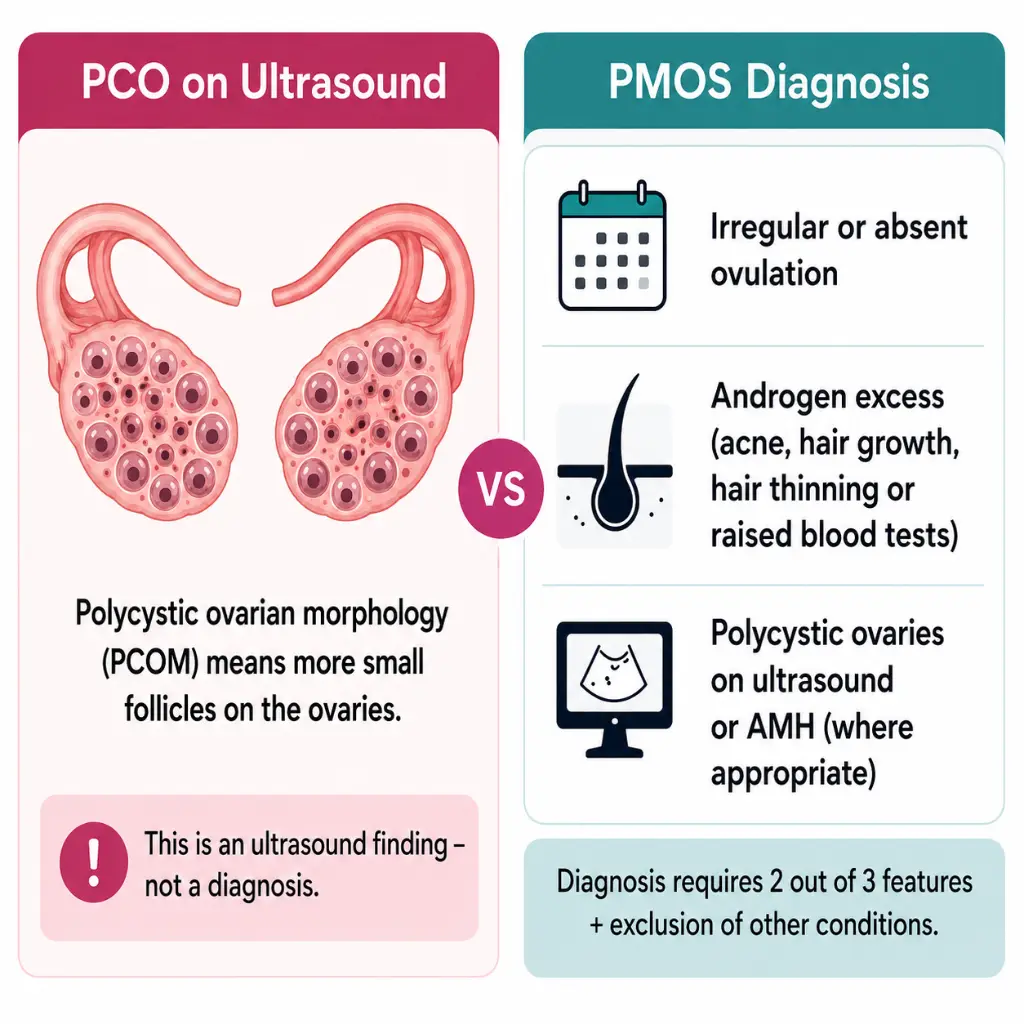
PMOS is usually diagnosed through a GP-led review using the Rotterdam criteria. In adults, diagnosis generally needs two out of three features: irregular or absent ovulation, clinical or biochemical androgen excess, and polycystic ovarian morphology on ultrasound or AMH where appropriate.
Do polycystic ovaries mean I have PMOS?
No. Polycystic ovaries, also called PCO or PCOM, describe how the ovaries look on ultrasound. They do not prove PMOS without cycle changes, androgen signs or blood results, and exclusion of similar conditions.
What tests are used for PMOS or PCOS in Australia?
Your GP may arrange hormone blood tests, metabolic screening, thyroid and prolactin checks, and pelvic ultrasound when useful. Some adults may also have AMH tested. The right tests depend on age, symptoms, medicines, contraception use and fertility goals.
PCOS was renamed PMOS in May 2026
On 12 May 2026, a Monash-led global consensus published in The Lancet recommended PMOS as the new name for PCOS. PMOS stands for polyendocrine metabolic ovarian syndrome. The new name better reflects that the condition can involve hormones, metabolism, ovaries, skin, cycle timing, mental wellbeing and long-term health.
The rename does not mean your previous PCOS diagnosis was wrong or that you need a new diagnosis only because the wording has changed. During the transition, Australian GP notes, referrals, ultrasound reports, pathology forms and health websites may use PCOS, PMOS or both terms.
Australian public health information is also moving through a transition period. Healthdirect now explains that PCOS was officially renamed PMOS in May 2026, while noting that Australian guidance and patient resources may continue using both names as updates roll out over coming years. RANZCOG has also welcomed the rename, which supports the use of both terms during the transition so patients can still recognise older records, referrals and test results.
Your GP is not required to change old records from PCOS to PMOS for the diagnosis to remain valid. If you are reading older Australian health resources, search both terms. For the full context behind the name change, read Fertility2Family’s PMOS rename guide for Australia. If you are speaking with a GP, ask whether your symptoms and test results meet the current diagnostic criteria and whether the PMOS wording changes anything in your care.
PCO vs PCOS vs PMOS: what is the difference?
PCO means polycystic ovaries. It describes how the ovaries look on ultrasound and is not a diagnosis by itself. PCOS is the older name for the condition. PMOS is the new name for the same condition.
This difference matters because a scan can show polycystic ovarian morphology when cycles are regular and androgen blood tests are normal. That scan result alone may not mean PMOS. The reverse can also happen. A person may have PMOS with a normal ultrasound if irregular ovulation and androgen excess are present after similar conditions have been considered.
This is why the diagnostic pathway should be read alongside what the 2026 rename means for Australian women. The name has changed, but the diagnosis still depends on the full clinical pattern.
The Rotterdam diagnostic criteria, explained
In adults, PMOS is usually assessed using the same diagnostic framework used for PCOS. The Rotterdam criteria look for two out of three features after similar conditions have been considered: irregular or absent ovulation, clinical or biochemical androgen excess, and polycystic ovarian morphology on ultrasound or AMH.
Under the 2023 International PCOS Guideline, AMH may be used instead of ultrasound to define the ovarian morphology feature in some adults, but AMH is not a stand alone diagnostic test.
For example, cycles every 45 to 70 days plus raised free testosterone may be enough for diagnosis if other causes are checked and no better explanation is found. A scan showing polycystic ovaries with regular cycles and normal androgen results does not confirm PMOS.
What your GP is looking for
Ovulation may be irregular when periods are unpredictable, cycles are often longer than 35 days, cycles are shorter than 21 days, or there are fewer than eight cycles per year after the early years following the first period. A period-like bleed does not always prove ovulation happened.
Clinical androgen excess means signs such as persistent adult acne, unexpected facial or body hair growth, or scalp hair thinning. Biochemical androgen excess means blood tests show raised androgens, such as testosterone, calculated free androgen index or DHEAS.
Seek prompt medical advice if androgen symptoms change suddenly, become severe, or appear with voice deepening, rapid scalp hair loss or marked body changes. These patterns are not typical of gradual PMOS and need medical review.
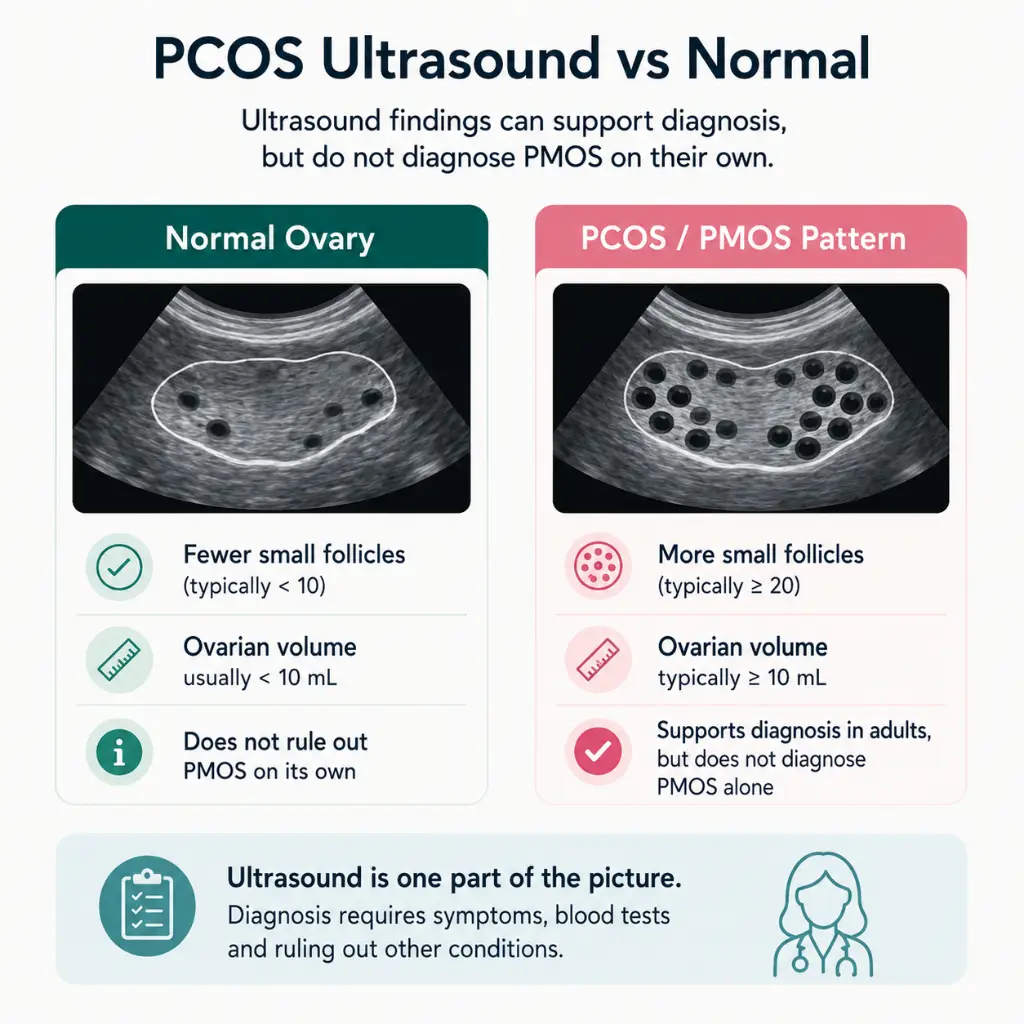
Polycystic ovarian morphology means the ovaries show more small follicles or increased ovarian volume. The 2023 International PCOS Guideline updated the adult ultrasound threshold to 20 or more follicles per ovary in at least one ovary. Ovarian volume of 10 mL or more may also be used. The older “12 follicles” threshold is no longer the preferred adult standard.
The Australian GP pathway for PMOS diagnosis
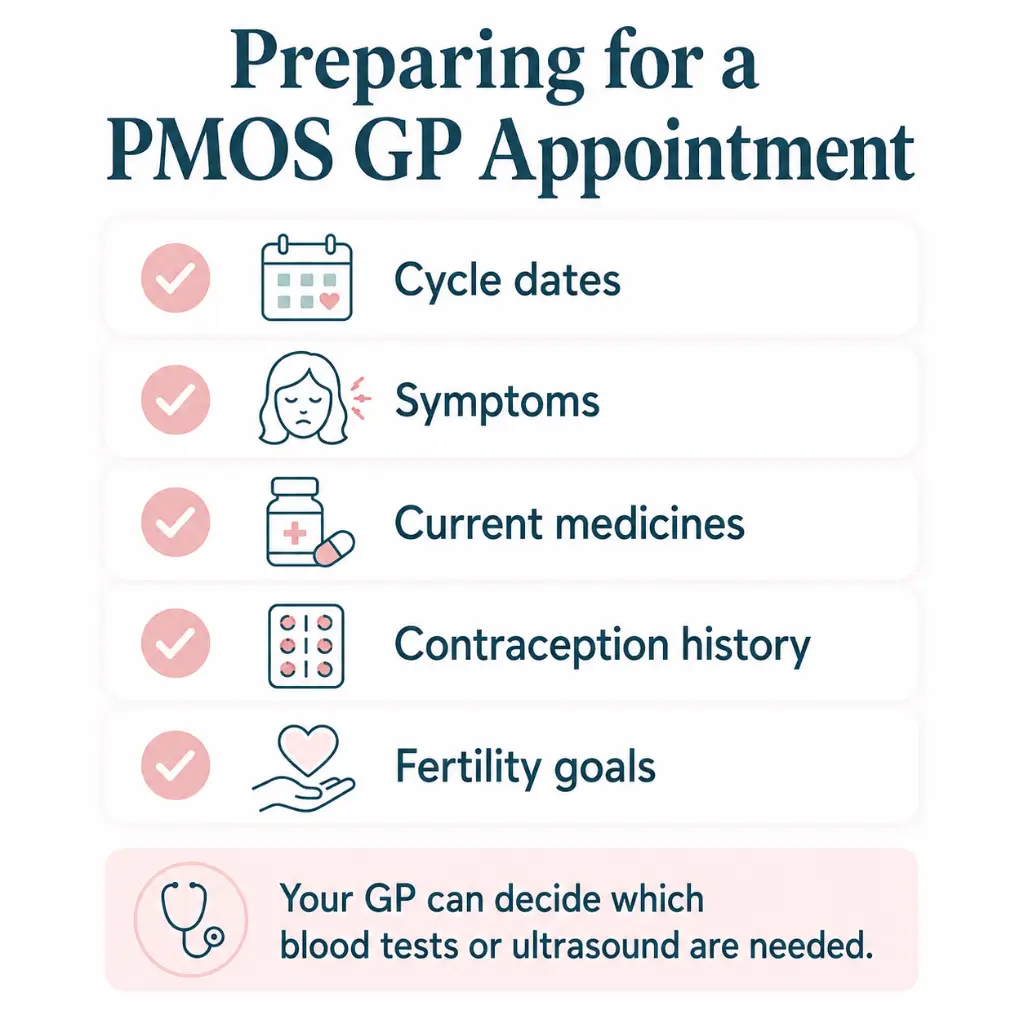
In Australia, the usual starting point is a GP appointment. Your GP can review your cycle pattern, symptoms, medicines, contraception use, family history, fertility goals and metabolic risk.
Your GP may ask about period timing, cycle length and regularity, the age your periods first started, acne history, facial or body hair growth, scalp hair thinning, weight change, family history of PCOS or PMOS, mental health history and whether you are trying to conceive. They may also check blood pressure and discuss metabolic screening. PMOS care should not reduce the condition to weight.
This also fits with the wider Australian women’s health policy direction in 2025 and 2026, which has placed more attention on access to reproductive and gynaecological care. The Australian Government reported new Medicare-supported services for complex gynaecological conditions, including PCOS, endometriosis and chronic pelvic pain. These policy changes do not alter the diagnostic criteria for PMOS, but they reinforce why persistent cycle, androgen, metabolic or fertility concerns should be raised with a GP rather than managed through self-testing alone.
Metabolic screening matters because insulin resistance can sit alongside PMOS, even when weight is not the main concern. If that is part of your review, read our separate guide to PMOS and insulin resistance in Australia.
From there, your GP may order blood tests, request pelvic ultrasound, arrange follow-up, or refer you to a gynaecologist, endocrinologist or fertility specialist.
Blood tests your GP may order
Blood tests for PMOS usually check androgen levels, ovulation related hormones and metabolic health. They also help rule out conditions that can look similar.
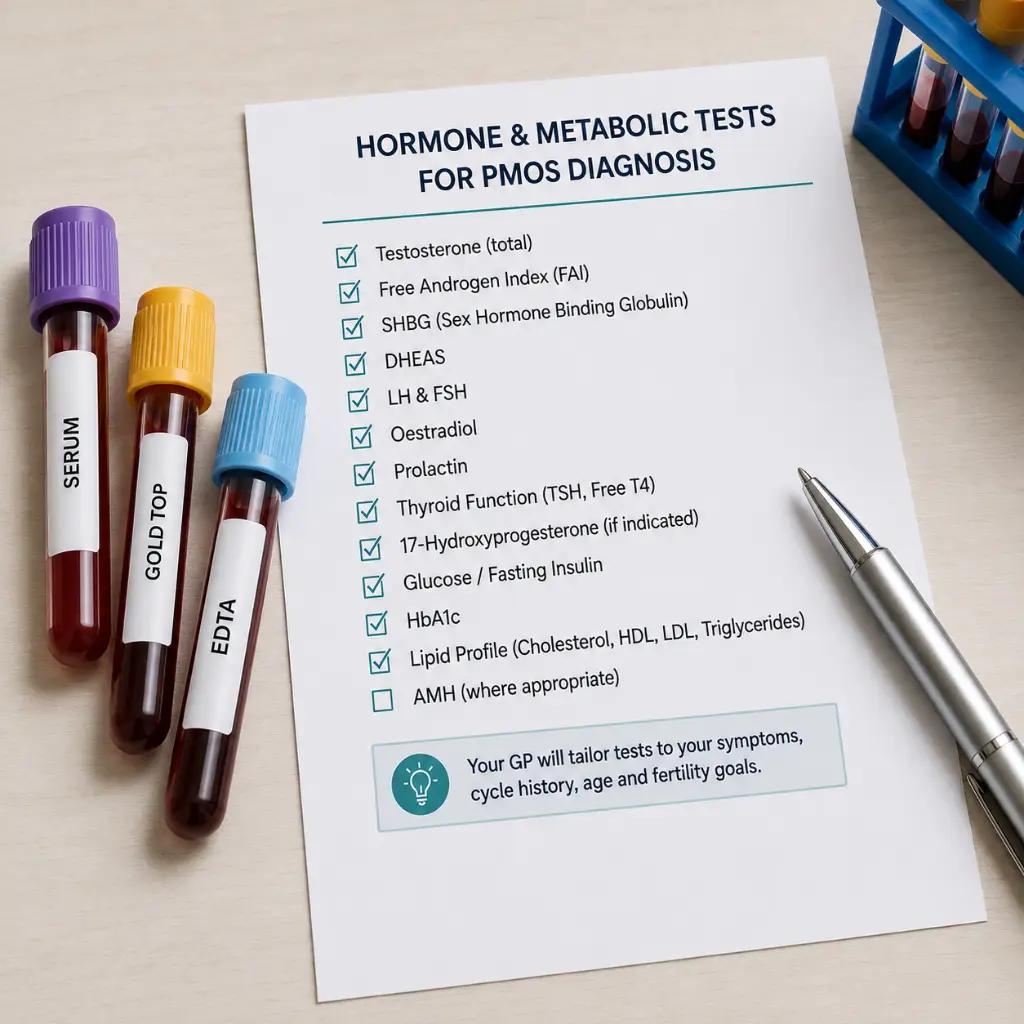
Your GP may order testosterone, calculated free androgen index, sex hormone binding globulin, DHEAS, FSH, LH, oestradiol, thyroid function, prolactin, fasting glucose, HbA1c and cholesterol. Some people may also need 17-hydroxyprogesterone, progesterone testing, an oral glucose tolerance test, or AMH.
Not everyone needs every test. The correct blood panel depends on your symptoms, age, cycle pattern, medicines, contraception use, family history and whether another condition needs to be ruled out. Progesterone is usually checked about seven days after suspected ovulation, not simply on day 21 for every person. AMH can often be checked on any cycle day, but it still needs clinical interpretation.
Medicare rebates may apply to GP-requested pathology when tests are clinically needed, but billing varies. If a pathology test is bulk billed, Medicare pays the full cost and there is no out of pocket fee for that test. If it is not bulk billed, you may need to pay a gap or private fee.
Large pathology providers vary by state and region. For example, people may see providers such as Laverty Pathology or Douglass Hanly Moir in New South Wales, Dorevitch Pathology or Melbourne Pathology in Victoria, QML Pathology or Sullivan Nicolaides Pathology in Queensland, Clinpath or SA Pathology in South Australia, Western Diagnostic Pathology or Clinipath Pathology in Western Australia, and TML Pathology in Tasmania. These examples do not guarantee bulk billing. Ask the GP clinic or collection centre whether each requested test is Medicare rebatable, bulk billed, or likely to involve an out of pocket cost.
Pelvic ultrasound: what to expect in Australia
A pelvic ultrasound may check follicle number, ovarian volume, endometrial thickness, uterine findings and other ovarian findings. It can support diagnosis in adults, but it does not diagnose PMOS by itself.
The scan may be transabdominal, transvaginal or both. A transabdominal scan uses a probe across the lower belly. A transvaginal scan uses a slim internal probe and can give a closer view of the ovaries when suitable and consented to.
Ask what type of scan is planned, whether you need a full bladder, whether you can stop at any time, and whether a female sonographer is available. Early follicular phase timing can make the scan easier to interpret.
Ultrasound is not usually needed at every PMOS review. It may be repeated if symptoms change, bleeding becomes concerning, endometrial protection is in question, or another pelvic issue needs checking.
PMOS ultrasound vs a normal ultrasound: what radiologists look for
A normal ultrasound report may describe ovaries without raised follicle number, without increased ovarian volume, and without other pelvic findings that need follow-up. A PMOS-pattern ultrasound may describe polycystic ovarian morphology, sometimes written as PCOM, with many small follicles or increased ovarian volume.
The report may also mention endometrial thickness. This does not diagnose PMOS by itself, but it can matter when periods have been absent for long stretches because the uterine lining may need protection. Your GP can interpret the ultrasound with your symptoms, cycle pattern and blood results.
A scan that says PCO, PCOM or polycystic ovarian morphology should not be read in isolation. It is one piece of the diagnostic pattern, not the whole diagnosis.
AMH as a diagnostic alternative or adjunct
AMH, or anti-Müllerian hormone, can reflect the number of small follicles in the ovaries. Under the 2023 International PCOS Guideline, AMH may be used instead of ultrasound to define the ovarian morphology feature in some adults.
AMH should not be used as a stand alone test for PMOS or to diagnose PMOS in adolescents. Results can vary by age, test method and clinical context. For a deeper explanation of cost, Medicare, timing and interpretation, read our guide to AMH testing for PCOS and PMOS in Australia.
Do I have PMOS? When to book the GP review
Book a GP review if your periods are often longer than 35 days apart, absent for months, unpredictable, very heavy, or paired with persistent adult acne, unexpected facial or body hair growth, scalp hair thinning, difficulty conceiving or repeated unclear ovulation patterns.
If you are unsure whether your symptoms fit the pattern, compare them with our PMOS symptoms guide for Australia. Symptoms alone do not prove PMOS, but they can help you explain the pattern clearly at your appointment.
Do not wait for a routine appointment if androgen symptoms change suddenly, become severe, or appear with voice deepening, rapid scalp hair loss or marked body changes. Those patterns need prompt medical review because they are not typical of gradual PMOS.
PMOS diagnosis in adolescents, on the pill and after pregnancy
PMOS diagnosis is more cautious in adolescents because puberty can naturally involve irregular cycles, acne and changing ovarian appearance. In adolescents, ultrasound morphology and AMH are not recommended for diagnosis. Diagnosis usually requires both ovulatory dysfunction and clinical or biochemical androgen excess, with other causes considered.
The combined oral contraceptive pill can make PMOS harder to assess because it can regulate bleeding, improve acne and alter androgen blood results. If androgen blood testing is needed while you are on the pill, your GP may discuss pausing the pill for at least three months and using another contraception method. Do not stop contraception without a plan if pregnancy prevention matters.
Cycle irregularity can be normal after pregnancy and while breastfeeding. Australian public guidance does not give one fixed timing rule for postpartum PMOS assessment. Your GP can interpret symptoms in context, especially if irregular cycles, androgen signs or metabolic concerns existed before pregnancy or continue after breastfeeding reduces or stops.
Conditions that look like PMOS but are not
Several conditions can cause irregular cycles, acne, hair changes or abnormal blood results. This is why PMOS diagnosis includes checking for other causes.
Thyroid disorders can change cycle timing and bleeding. Prolactin changes can reduce ovulation and cause missed periods. Hypothalamic amenorrhoea can occur with undernutrition, high exercise load, stress or weight change.
Premature ovarian insufficiency can cause irregular or absent periods, often with higher FSH and lower ovarian reserve markers. Non-classic congenital adrenal hyperplasia can raise adrenal androgens. Rare causes, such as Cushing’s syndrome or androgen-secreting tumours, need medical review when symptoms are sudden, severe or atypical.
Diagnostic delay and when to ask for referral
Delayed PCOS diagnosis has been documented in the medical literature and is one reason the PMOS rename matters. The old name could make the condition sound like an ovarian cyst problem, when diagnosis depends on a wider hormone, ovulation and metabolic pattern.
If you feel dismissed, ask which diagnostic criteria have been considered. You can ask whether your cycle pattern, androgen signs, androgen blood tests, ultrasound results and rule-out tests have been reviewed together. You can also ask your GP to record the plan, arrange follow-up after test results, or explain why PMOS is unlikely. If symptoms persist and no clear plan is made, a second GP opinion is reasonable.
Your GP may refer you if the diagnosis is uncertain, symptoms are severe, androgen levels are very high, periods are absent for long periods, fertility treatment may be needed, or another condition needs to be ruled out. An endocrinologist may help with hormone or metabolic features, a gynaecologist with bleeding or pelvic symptoms, and a fertility specialist if pregnancy is the goal.
If pregnancy is your main concern, keep this diagnostic page focused on confirming the pattern first, then read our separate guide to PMOS fertility and pregnancy in Australia.
What happens after PMOS is diagnosed?
After diagnosis, care depends on symptoms, fertility goals and metabolic risk. Your GP may discuss cycle regulation, skin or hair symptoms, metabolic screening, mental health, contraception, preconception care or referral.
Follow-up may include blood pressure, glucose or diabetes risk checks, cholesterol checks, mental health screening, sleep apnoea screening where relevant, and endometrial protection if periods are often absent.
Receiving a PMOS diagnosis can bring relief, confusion or distress. Anxiety and depression are more common in PCOS and PMOS than in the general population, and mental health support is part of holistic PMOS management. Your GP can discuss counselling, psychology referral or a mental health treatment plan if symptoms are affecting daily life.
This page does not cover diet, insulin resistance, inositol dosing or fertility prognosis in depth because those topics need separate pages. If nutrition is your next question after diagnosis, read our guide to PCOS and PMOS diet in Australia.
PMOS and fertility tracking
PMOS can make ovulation harder to predict when cycles are irregular. Some people have delayed ovulation, multiple patches of fertile-looking mucus, or LH results that do not match their cycle pattern.
Ovulation tests may help if you can identify a reasonable testing window. If cycles are long or unpredictable, ovulation test strips can be useful for extended-window tracking. They still do not diagnose PMOS or prove ovulation by themselves.
Pregnancy tests work the same in people with PMOS, but late ovulation can make testing too early more likely. If your period is absent and tests remain negative, book a GP review. If you are testing after delayed ovulation, pregnancy test strips can help you test over several days without relying on one early result.
Frequently Asked Questions About PMOS Diagnosis Australia
What is PCO full form?
PCO usually stands for polycystic ovaries. In scan language, PCOM means polycystic ovarian morphology. These terms describe ovarian appearance on ultrasound and do not prove PMOS without the wider clinical pattern.
Can PMOS be diagnosed without ultrasound?
Yes. In adults, PMOS may be diagnosed without ultrasound if irregular ovulation and androgen excess are present and other causes have been considered. AMH may also be used instead of ultrasound in some adult diagnostic pathways, but not as a stand alone test.
What blood tests are used to diagnose PMOS or PCOS in Australia?
Blood tests may include testosterone, free androgen index, sex hormone binding globulin, DHEAS, FSH, LH, thyroid function, prolactin, glucose testing, HbA1c, cholesterol and sometimes AMH or 17-hydroxyprogesterone.
How is PMOS diagnosed if I am on the pill?
The pill can mask cycle pattern and alter androgen blood results. If biochemical androgen assessment is needed, your GP may discuss pausing the pill for at least three months with another contraception plan.
When should I see a GP about possible PMOS?
See a GP if your cycles are often longer than 35 days, absent for months, unpredictable, very heavy or very painful. Also seek advice for persistent adult acne, unexpected facial or body hair growth, scalp hair thinning, difficulty conceiving, or symptoms that changed suddenly.
How much does PMOS testing cost in Australia?
Costs vary. GP consultations, pathology and ultrasound may be bulk billed or may involve gap fees. AMH is more likely to have an out of pocket cost. Ask your GP clinic or pathology collection centre whether the requested tests are bulk billed before collection.
Next Steps in Australia
If your ultrasound report mentions PCO, PCOM or polycystic ovarian morphology, book a GP appointment and bring your cycle dates, symptoms, medicines and contraception history. Ask whether your pattern meets diagnostic criteria and whether blood tests or ultrasound are needed.
If you are tracking cycles while waiting for review, ovulation tests, cervical mucus notes, basal body temperature and pregnancy tests can help you collect information. They should support GP review, not replace it.
Last reviewed: May 19, 2026
Next scheduled review: May 2027
References
Fertility2Family publishes Australia-focused fertility education. Articles are written by our team and medically reviewed by Australian-registered health practitioners. We use Australian consumer medicine information, Australian clinical and public health guidance, and peer-reviewed research consistent with Australian care. We explain what the evidence suggests, what it cannot confirm, and when to see a GP or fertility specialist. Each article lists its author, medical reviewer, and review dates.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00717-8/fulltext
https://www1.racgp.org.au/newsgp/clinical/pcos-officially-renamed-polyendocrine-metabolic-ov
https://www.monash.edu/medicine/mchri/pcos/guideline
https://academic.oup.com/jcem/article/108/10/2447/7242360
https://www.servicesaustralia.gov.au/bulk-billing?context=60092
https://www.dorevitch.com.au/patients/billing-policy
https://www.tmlpath.com.au/patients/medicare-rebate
https://www.jeanhailes.org.au/health-topics/pcos/
https://www.healthdirect.gov.au/polycystic-ovarian-syndrome-pcos
https://www.healthdirect.gov.au/paying-for-diagnostic-testing
https://www.healthdirect.gov.au/understanding-pathology-tests
https://www.health.qld.gov.au/cpc/gynaecology/polycystic-ovarian-syndrome-pcos
https://www.racgp.org.au/afp/2012/october/polycystic-ovary-syndrome
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/polycystic-ovarian-syndrome-pcos


