
An AMH test can contribute to PCOS or PMOS diagnosis in selected adults, but a high AMH result cannot diagnose the condition by itself. PMOS, polyendocrine metabolic ovarian syndrome, is the new name for the condition previously called PCOS. The name changed in May 2026; the diagnostic criteria and treatment did not.
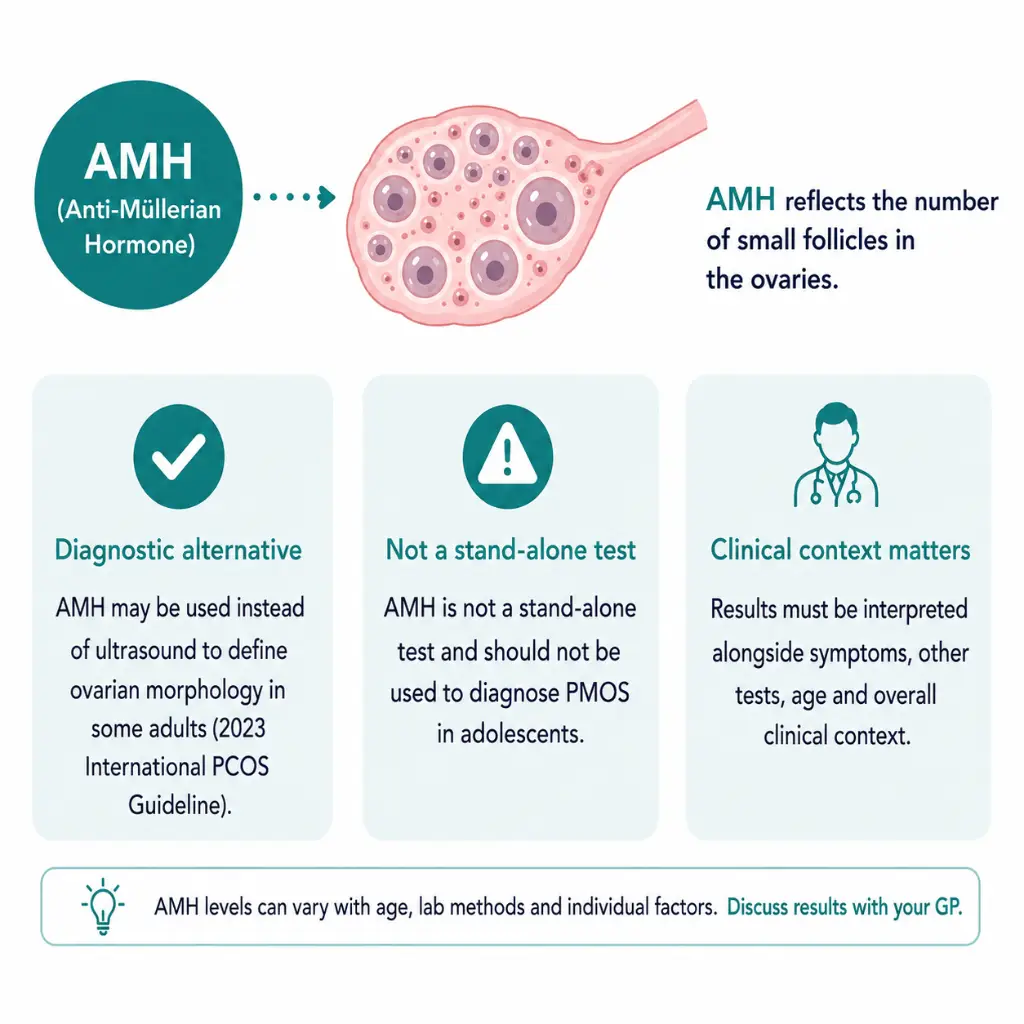
Under the Australian-led 2023 international guideline, anti-Müllerian hormone may be used as an alternative to pelvic ultrasound for the polycystic-ovarian-morphology part of adult diagnosis when that criterion is needed. If irregular cycles and hyperandrogenism are already present, neither AMH nor ultrasound is usually required to establish the diagnosis after other causes have been considered. AMH and ultrasound should not be added together simply to confirm the same criterion, and neither test is recommended for diagnosing PMOS in adolescents.
This guide explains how PMOS is tested in Australia, where AMH fits in the diagnostic pathway, what a low or high result can and cannot mean, how pathology billing works, and what to discuss with a GP or fertility specialist.
Quick Answers About AMH Tests for PCOS and PMOS
How do you test for PMOS in Australia?
There is no single PMOS blood test. Adult assessment combines cycle history, clinical or biochemical androgen excess and, when needed, ovarian morphology assessed with AMH or ultrasound, while considering other causes.
Can a high AMH result diagnose PCOS or PMOS?
No. In adults, AMH may support the ovarian-morphology criterion within the complete diagnostic algorithm. Cycle pattern, clinical or biochemical hyperandrogenism, exclusion of other causes and the reason for testing still matter.
Should AMH and ultrasound both be used for the same criterion?
Usually no. The guideline recommends ultrasound or AMH, not both, to define polycystic ovarian morphology in adults when that criterion is needed. An ultrasound may still be appropriate for a separate pelvic or structural concern.
Is AMH used to diagnose PMOS in teenagers?
No. AMH and ultrasound are not recommended for adolescent diagnosis because normal puberty can overlap with PMOS-like findings. Adolescent assessment uses age-appropriate menstrual and hyperandrogenism criteria.
The Adult PMOS Diagnostic Pathway
In adults, PMOS is diagnosed after other relevant causes are considered and at least two of the following three features are present:
- Clinical or biochemical hyperandrogenism, such as hirsutism or elevated androgens assessed with an appropriate laboratory method.
- Ovulatory dysfunction, usually reflected by irregular or absent ovulation and menstrual cycles.
- Polycystic ovarian morphology, assessed by pelvic ultrasound or, in selected adults, an appropriately interpreted AMH result.
| Clinical picture | Is AMH needed? | Reason |
|---|---|---|
| Irregular cycles plus clinical or biochemical hyperandrogenism | Usually no. | Two diagnostic features are already present after other causes are considered. Adding AMH may increase cost and confusion without changing the diagnosis. |
| Irregular cycles without clear hyperandrogenism | Possibly. | Ultrasound or AMH may be used to assess the ovarian-morphology criterion in an adult. |
| Hyperandrogenism with regular cycles | Possibly. | Ultrasound or AMH may help determine whether a second diagnostic feature is present. |
| High AMH with no symptoms or cycle concern | Not diagnostic. | A high result can occur without PMOS and should not create a diagnosis by itself. |
| Adolescent with irregular cycles or acne | No diagnostic AMH. | Pubertal physiology overlaps with PMOS. Adolescent criteria and follow-up are different. |
A clinician also considers other explanations for irregular cycles or androgen excess. The investigations are tailored to the history rather than being identical for everyone. For the complete criteria and exclusion process, see how PMOS is diagnosed in Australia.
How to Test for PMOS in Australia: Blood Tests, AMH and Ultrasound
There is no single blood test for PMOS. The diagnostic criteria are assessed through a combination of cycle history, clinical examination and selected tests. AMH answers only the ovarian-morphology question in selected adults; it does not replace androgen assessment or the consideration of other causes.
| Part of the assessment | What may be checked | What it helps answer |
|---|---|---|
| Cycle and ovulation pattern | Menstrual history and, when needed, additional ovulation assessment selected by the clinician. | Whether ovulatory dysfunction or irregular cycles are present. |
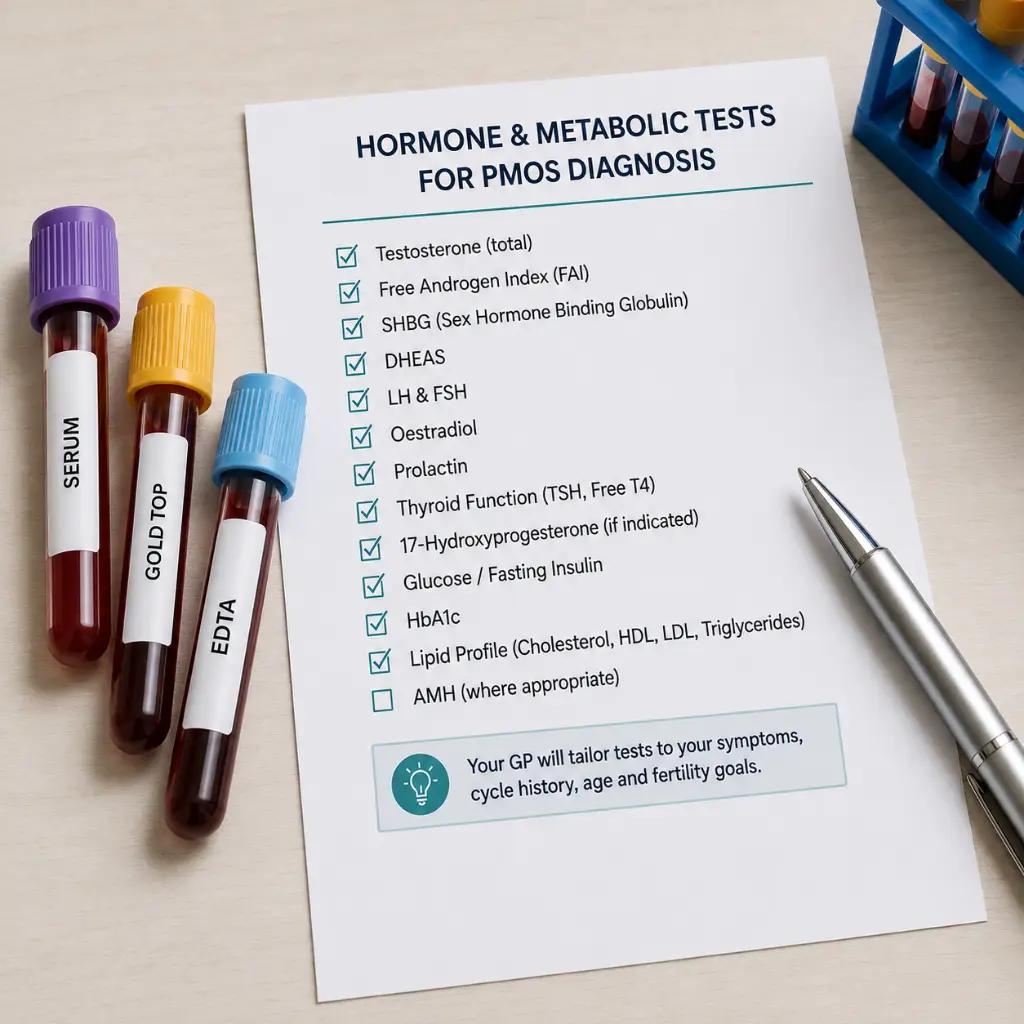
| Clinical or biochemical hyperandrogenism | Symptoms such as hirsutism and/or total and free testosterone. Additional androgen testing may be considered when clinically appropriate. | Whether the androgen criterion is present. |
| Ovarian morphology | AMH or pelvic ultrasound, not both automatically, in selected adults when this criterion is needed. | Whether ovarian morphology supports the diagnosis. |
| Other possible causes | Targeted tests may include thyroid function, prolactin, 17-hydroxyprogesterone, FSH or other investigations based on the presentation. | Helps consider conditions that can mimic PMOS. Not every person requires every test. |
| Metabolic health | Blood pressure, glucose assessment and lipids, according to clinical context. | Identifies associated health risks and guides management. These are not the two-of-three diagnostic features. |
PMOS blood tests are selected to answer different clinical questions rather than ordered as one universal panel. Hormonal contraception can affect androgen testing and AMH interpretation, so tell the clinician what you use before testing. The wider Australian PMOS diagnostic guide explains the complete work-up and exclusion pathway.
What AMH Measures and Why It May Be High in PMOS
Anti-Müllerian hormone is produced by granulosa cells around small developing ovarian follicles. The blood result is associated with the number and activity of these follicles, but it is not a literal egg count and does not show whether an egg was released in the current cycle.
Many people with PMOS have more small follicles and may therefore have a higher AMH concentration. This association is why AMH can help represent polycystic ovarian morphology in selected adults. Association is not identity: a high result can occur without PMOS, and a person can meet PMOS criteria without having a high AMH result.
Age, the laboratory assay, hormonal contraception, pregnancy, ovarian surgery, chemotherapy and individual biology can influence interpretation. The result should be read with the reporting laboratory’s reference information and the person’s clinical picture.
AMH or Ultrasound: Not Automatically Both
Pelvic ultrasound and AMH are two ways of assessing the ovarian-morphology component in the adult diagnostic algorithm. Using both for that same criterion can duplicate evidence and increase the risk of overdiagnosis without improving the decision.
Ultrasound may still be needed for another clinical reason, such as pelvic pain, abnormal bleeding, suspected fibroids, an ovarian mass or another structural question. In that situation, the scan is not being ordered merely to repeat the AMH criterion.

How AMH Testing and Billing Work in Australia
AMH is measured from a blood sample using a laboratory immunoassay. Australian pathology guidance states that reference intervals depend on age and the testing method, so use the range and notes supplied by the reporting laboratory rather than applying a general online chart.
Tell the requesting clinician about hormonal contraception and high-dose biotin supplements because these can affect interpretation. Do not stop contraception solely to obtain an AMH result without discussing pregnancy prevention and whether retesting would change care.
The Royal College of Pathologists of Australasia currently lists AMH as non-MBS rebatable, meaning there is no standard Medicare Benefits Schedule rebate for the test. A clinic or pathology provider may set its own private fee. Having a pathology request does not automatically make the test Medicare-rebatable or free, so confirm the current fee before collection.
- Ask whether the pathology service charges a separate AMH fee.
- Ask whether the GP or specialist appointment has an out-of-pocket cost.
- Ask how and when the result will be reviewed, particularly if PMOS diagnosis or fertility treatment is being considered.
There Is No Universal AMH Cut-Off for PCOS or PMOS
The international guideline does not endorse one AMH number that diagnoses PMOS in every laboratory, age group or population. Assays differ, AMH changes with age, and a value copied from an overseas chart may use a different method, unit or population.
A 2024 systematic review and meta-analysis included 82 studies. For adult PCOS diagnosis, pooled sensitivity was 79% and specificity was 87%, but study heterogeneity was substantial. The authors concluded that AMH alone is insufficient for diagnosis and that no international cut-off could be recommended.
The practical implication is straightforward: a laboratory flag or a result described as “high” is not a positive PMOS test. It becomes clinically useful only when interpreted inside the adult diagnostic pathway.

What a Low, Typical or High AMH Result Can Mean
- A lower result may indicate fewer small follicles relative to the laboratory’s age- and method-specific reference information. It does not rule out PMOS or prove that natural conception is impossible.
- A result within the laboratory range does not prove regular ovulation and does not rule out PMOS when other diagnostic features are present.
- A higher result may fit with a greater number of small follicles and can support the ovarian-morphology criterion in selected adults. It does not confirm PMOS by itself.
The most useful question is not whether the number is “good” or “bad”. Ask what clinical decision the result is meant to change and whether that decision belongs to PMOS diagnosis, ovarian-response planning or another question.
High AMH Is Not the Same as High Fertility
AMH can help estimate ovarian response during fertility treatment. It does not measure egg quality, prove regular ovulation, show that fallopian tubes are open, assess sperm or accurately predict natural conception for an individual person.
This distinction is particularly important in PMOS. A person may have a high AMH and many small follicles but ovulate infrequently. Another person can have a lower AMH and still ovulate and conceive. For ovarian-reserve and age-based interpretation, use the separate guide to AMH levels and fertility rather than treating diagnostic and fertility-prediction questions as the same issue.
Hormonal Contraception, Pregnancy and Other Contexts
Hormonal contraception can change cycle patterns, androgen assessment and AMH concentration. The effect is not identical for every method or person. A clinician may interpret the result cautiously or decide that another time or test is more useful.
Pregnancy can lower AMH concentration, and recent ovarian surgery, chemotherapy or marked suppression of ovarian function can also change the relevance of a result. An AMH test is not a pregnancy test and is not used to assess pregnancy viability.
Why Adolescents Need a Different Approach
Irregular cycles, acne and high follicle numbers can occur during normal puberty. Using AMH or ultrasound too early can overdiagnose a long-term condition. Adolescent diagnosis requires persistent menstrual irregularity defined by time since menarche plus clinical or biochemical hyperandrogenism after relevant alternatives are considered.
A teenager who has symptoms but does not yet meet both criteria may be considered at increased risk and followed over time. Symptom support does not need to wait for a premature diagnosis.
AMH Does Not Select Treatment by Itself
A high AMH result does not automatically mean that ovulation medicine, IVF or a particular dose is required. Treatment depends on the person’s goals, ovulation pattern, age, metabolic health, semen and tubal factors, duration of trying and previous response.
During fertility treatment, AMH can help anticipate ovarian response and the risk of an excessive response, but clinics also use age, antral follicle count, previous stimulation and other clinical information. A medicine or dose should not be chosen from an online AMH chart.
What to Do With an AMH Result
| Situation | Useful next question | What to avoid |
|---|---|---|
| High AMH with irregular cycles or androgen symptoms | Does the complete adult PMOS algorithm support a diagnosis, and have other causes been considered? | Assuming the number alone confirms PMOS. |
| High AMH with regular cycles and no symptoms | Why was the test ordered, and would another assessment change care? | Creating a disease label from an incidental result. |
| AMH within the laboratory range with strong PMOS features | Do the other diagnostic features meet the criteria? | Using the AMH result to rule out PMOS. |
| Lower AMH with possible PMOS | Are PMOS diagnosis and ovarian-reserve interpretation being confused? | Assuming lower AMH excludes PMOS or makes conception impossible. |
| AMH measured while using hormonal contraception | Could the method affect interpretation, and would retesting change management? | Stopping contraception without a clinical and pregnancy-prevention plan. |
| AMH ordered for general future-fertility reassurance | What can this result reliably answer, and what can it not predict? | Treating AMH as a countdown clock or natural-fertility score. |
When Retesting May, and May Not, Help
Frequent repeat AMH testing rarely adds value when no clinical decision has changed. Retesting may be considered when the original result was obtained in a context that limits interpretation, a laboratory or sample issue is suspected, or updated information would change fertility-treatment planning.
If the goal is to determine whether ovulation is occurring, use cycle history and appropriate ovulation assessment rather than repeated AMH. The PMOS ovulation-tracking guide explains why LH tests can be difficult to interpret and how to combine tracking methods.
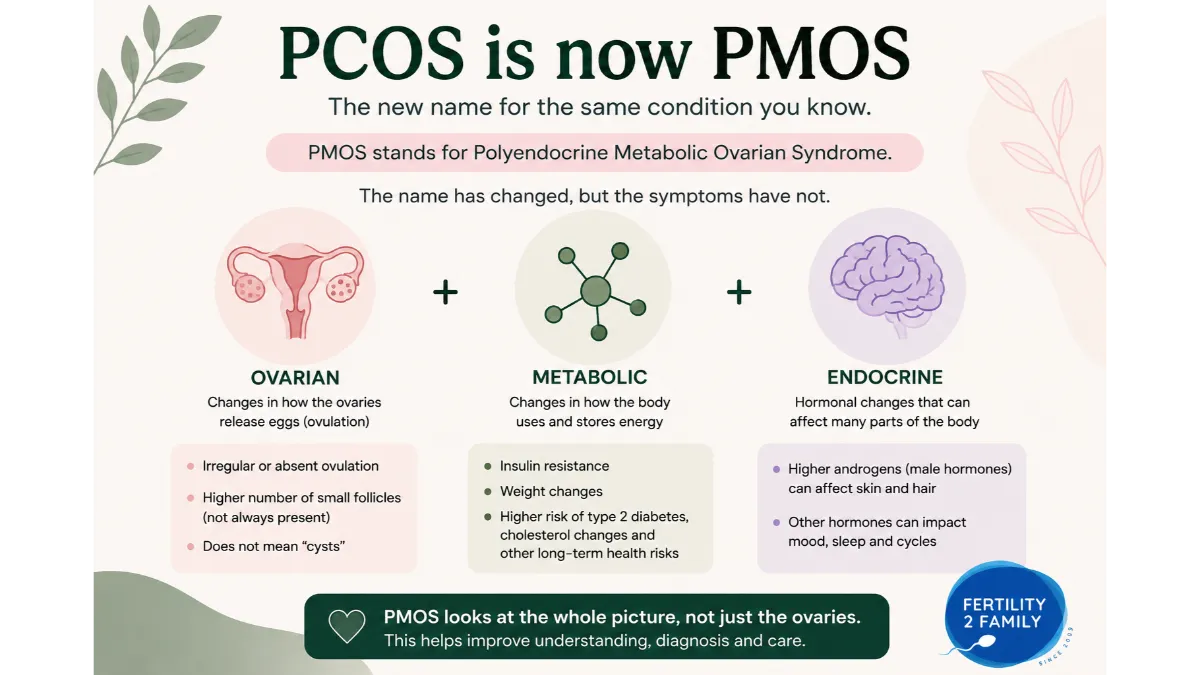
The 2026 Name Change: PMOS and PCOS Mean the Same Condition
In May 2026, polycystic ovary syndrome was renamed polyendocrine metabolic ovarian syndrome. The new name better reflects the condition’s endocrine, metabolic and ovarian features and removes the misleading focus on ovarian “cysts”.
A planned transition means that PCOS will remain common in searches, medical records, pathology forms and published research while PMOS terminology is implemented. The international guideline update planned for 2028 is expected to complete the formal transition. The diagnosis and treatment did not change because of the name change.
For a broader explanation, see the PCOS-to-PMOS name change in Australia. For symptom patterns and GP preparation, use PMOS symptoms in Australia.
Frequently Asked Questions About AMH Tests and PMOS Diagnosis in Australia
What does PMOS stand for, and is it different from PCOS?
PMOS stands for polyendocrine metabolic ovarian syndrome. It is the new name for the condition previously called PCOS. The diagnostic criteria and treatment did not change.
What blood tests are used to check for PMOS?
There is no universal blood-test panel. Depending on symptoms and medicines, a clinician may assess androgens and arrange targeted tests such as thyroid function, prolactin, 17-hydroxyprogesterone or FSH to consider other causes. AMH is used only for the ovarian-morphology criterion in selected adults.
Can a normal AMH result rule out PMOS?
No. PMOS can be diagnosed through other combinations of adult criteria, and AMH varies with age, assay and clinical context. A result within the laboratory range should not override persistent cycle or androgen features.
Is there one AMH cut-off for PMOS diagnosis?
No. Assays, age groups and populations differ. The result must be interpreted with the laboratory method and the complete adult diagnostic criteria.
Does Medicare cover AMH testing in Australia?
The Royal College of Pathologists of Australasia currently lists AMH as non-MBS rebatable, so there is no standard Medicare Benefits Schedule rebate for the test. Providers may set different private fees, so confirm the current out-of-pocket cost before collection.
Does high AMH mean I am more fertile?
No. It may reflect more small follicles or predict a stronger response to ovarian stimulation, but it does not measure egg quality, prove ovulation or accurately predict natural conception.
Does the contraceptive pill affect AMH?
Oral and other hormonal contraception can affect AMH interpretation in some people and can also change cycle and androgen assessment. Discuss whether the result is useful before stopping contraception.
When should AMH be repeated?
Routine frequent retesting is usually unhelpful. It may be considered when the original context limited interpretation, a sample or laboratory issue is suspected, or updated information would change fertility-treatment planning.
Next Steps in Australia
Take the complete AMH report, including the units, reporting laboratory and collection date, to a GP or fertility specialist. Also bring a list of medicines and supplements. Ask which diagnostic feature the test is meant to assess, whether the other adult PMOS criteria are present, whether other causes need consideration and whether ultrasound would duplicate the same criterion.
If PMOS is confirmed, the next plan should address the person’s priorities, including cycle symptoms, metabolic health, skin or hair changes, mental health, contraception or conception. The PMOS and insulin-resistance guide covers metabolic assessment, while fertility and pregnancy with PMOS covers conception planning.
Last reviewed: 31 July 2026
Next scheduled review: July 2027
References
Fertility2Family articles are researched using Australian Government health guidance, professional clinical recommendations and peer-reviewed medical literature. The references below were used to research and medically review this article and provide additional reading for readers who want to explore the evidence in more detail.
Monash University.
PCOS Guideline/ PMOS Guideline
Provides the Australian-led international diagnostic and management framework, including adult AMH use, adolescent exclusions, clinical algorithms, shared decision-making and evidence-based care resources.
Medical Journal of Australia.
Summary of the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome: an Australian perspective
Summarises the NHMRC-approved Australian-led guideline, including the adult two-of-three diagnostic framework, AMH as an ultrasound alternative and distinct criteria for adolescents.
Royal College of Pathologists of Australasia.
Anti-Mullerian hormone
Provides Australian pathology guidance on specimens, immunoassay testing, method-dependent reference intervals, oral contraceptive and biotin effects, clinical uses and non-MBS-rebatable status.
Explains Australian professional support for the 2026 PCOS-to-PMOS name change and the planned transition while clinical criteria and treatment remain unchanged.
Reports the global consensus process behind the PMOS name, involving patients and health professionals, and outlines scientific, communication and implementation principles for the transition.
Journal of Clinical Endocrinology & Metabolism.
Recommendations From the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome
Presents the guideline recommendations and diagnostic algorithm, including AMH as an adult ultrasound alternative, exclusion of other causes and limits on adolescent use.
Fertility and Sterility.
Anti-müllerian hormone as a diagnostic biomarker for polycystic ovary syndrome and polycystic ovarian morphology: a systematic review and meta-analysis
Synthesises 82 studies of AMH diagnostic performance, finding useful adult accuracy but substantial heterogeneity, insufficient stand-alone specificity and no support for one international cut-off.
American Journal of Obstetrics & Gynecology.
Anti-Müllerian hormone as a diagnostic marker of polycystic ovary syndrome: a systematic review with meta-analysis
Evaluates AMH diagnostic performance across 45 studies and concludes that age, assay standardisation, body mass index and PMOS phenotype must inform interpretation.
European Journal of Endocrinology.
Should anti-Müllerian hormone be a diagnosis criterion for polycystic ovary syndrome? An in-depth review of pros and cons
Reviews benefits and limitations of AMH in adult diagnosis, including assay variation, threshold uncertainty, age effects, phenotype differences and concerns about adolescent testing.
Frontiers in Endocrinology.
Variation in the Measurement of Anti-Müllerian Hormone – What Are the Laboratory Issues?
Explains laboratory sources of AMH variation, including calibration, antibody design, isoforms, analytical interference and between-method differences that limit direct comparison of results.
Fertility and Sterility.
Contraceptive-specific antimüllerian hormone values in reproductive-age women: a population study of 42,684 women
Examines AMH distributions across contraceptive methods and ages, showing method-specific population effects and supporting cautious interpretation when hormonal contraception is being used.
Reproduction and Fertility.
Serum anti-müllerian hormone (AMH) concentration during pregnancy: a longitudinal study
Reports an Australian longitudinal cohort showing AMH commonly decreased from the first to second trimester, supporting caution when interpreting results obtained during pregnancy.
Australian Journal of General Practice.
Assessment of female fertility in the general practice setting
Outlines Australian general-practice fertility assessment, including ovulation, ovarian reserve, pelvic anatomy, preconception care and the role of referral when further evaluation is required.