15 min read
Jul 9, 2026
How to Track Ovulation With PCOS or PMOS
Written by
Fertility2Family Team

Medically reviewed by
Evan Kurzyp, RN, BSN, Master of Nursing
AHPRA registration: NMW0002424871
Yes, you can track ovulation with PCOS or PMOS, but it is more accurate to use several signs together. Ovulation tests can show an LH rise, cervical mucus can suggest rising oestrogen, and BBT can help show whether ovulation likely happened afterwards. If cycles are irregular, a GP can arrange progesterone testing or ultrasound when needed.
This guide explains how to track ovulation with PCOS in Australia, why ovulation tests can be harder to read, what repeated positive or negative results can mean, and when home tracking should be checked with a GP.
Quick answers about tracking ovulation with PCOS or PMOS
How do I track ovulation with PCOS?
Use more than one sign. Ovulation tests can show a likely LH rise, cervical mucus can suggest rising oestrogen, and BBT can support that ovulation likely happened afterwards. If your cycles are irregular or results keep changing, speak with your GP.
Are ovulation tests accurate with PCOS?
Ovulation tests can be useful with PCOS, but they may be harder to interpret. Some people have higher baseline LH, delayed ovulation, repeated positive tests or no clear surge. The result is more useful when read with cycle dates, mucus and BBT.
Can you ovulate with PCOS and irregular cycles?
Yes. Some people with PCOS ovulate regularly, some ovulate later than expected, and some ovulate less often. Irregular cycles make prediction harder, but they do not mean ovulation never happens. A GP can arrange testing if ovulation remains unclear.
Why tracking ovulation with PCOS can be harder
Tracking ovulation with PCOS can be harder because ovulation may be delayed, irregular or absent in some cycles. LH tests, cervical mucus and cycle apps can still help, but they need to be read as a pattern rather than a single answer.
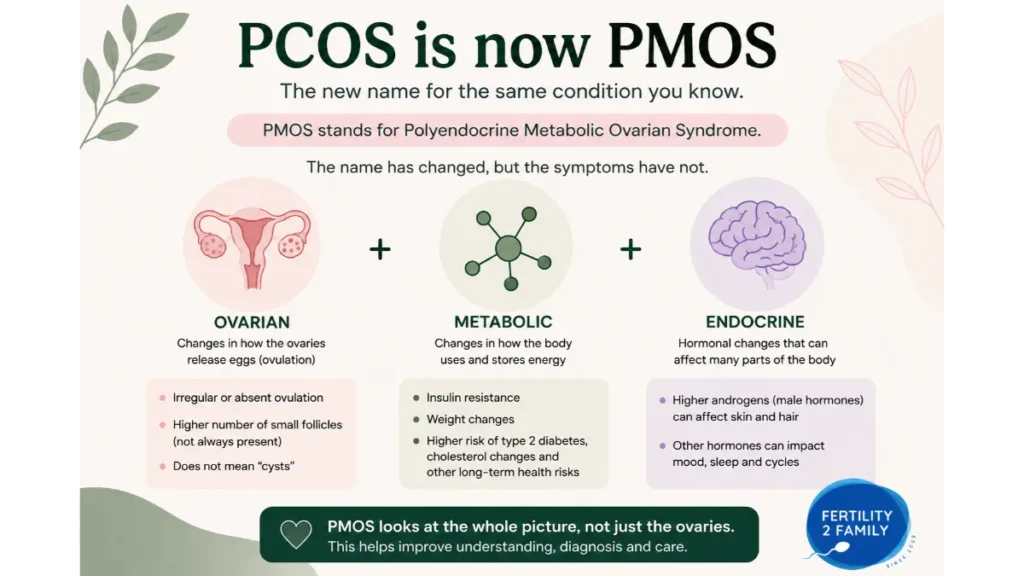
PCOS is now also being referred to as PMOS, or polyendocrine metabolic ovarian syndrome, in current Australian and international updates. During the transition, most people will still search for and hear the term PCOS. This article uses both terms so the information stays clear while the name change rolls out.
Ovulation usually happens when an egg is released from an ovary. With PCOS or PMOS, hormone patterns can make that release less predictable. Some people have long cycles, missed periods, repeated LH rises or fertile-looking mucus that does not lead to ovulation.
This is why one sign can mislead you. A positive ovulation test can suggest that ovulation may be approaching, but it does not confirm that an egg was released. If your cycles, skin, hair growth or metabolic symptoms suggest PCOS or PMOS, the broader symptom pattern also matters. Read more about PCOS symptoms now called PMOS in Australia.
How to use ovulation tests with PCOS
Ovulation tests with PCOS can help identify a likely LH rise when they are used consistently and read with your wider cycle pattern. They detect luteinising hormone in urine. They do not diagnose PCOS, PMOS, infertility, pregnancy or whether ovulation definitely happened.
If your cycles are predictable, start testing a few days before your expected fertile window. If your cycles are long or variable, you may need to start earlier or test for more days than someone with a regular 28-day cycle.
Test at a similar time each day and avoid drinking large amounts of fluid shortly before testing. Diluted urine can make a line appear lighter. Some people test twice daily near the expected fertile window because an LH surge can be short.
A simple pattern may look like this: cervical mucus becomes wetter over several days, an ovulation test turns clearly positive, then BBT rises and stays higher afterwards. With PCOS, that pattern may be less tidy. You may see mucus without a positive test, a positive test without a temperature rise, or more than one LH rise in the same cycle.
If you are testing across several days, ovulation tests can support repeated LH tracking when used exactly as directed. They are timing tools, not diagnostic tools.
Why ovulation tests can look always positive with PCOS
Repeated positive ovulation tests with PCOS can happen when baseline LH is higher, when the body makes more than one attempt to ovulate, or when LH rises without clear egg release. A positive ovulation test suggests timing, but it does not prove ovulation happened.
Some people describe this as an always positive ovulation test with PCOS. Others see several days of dark tests, a fade, then another dark result later in the cycle. This may reflect a delayed ovulation attempt, a second LH rise, or a hormone pattern that does not match ovulation.
A false positive ovulation test with PCOS can also happen when the test reads high LH but ovulation does not follow. This is why the result needs context. Stretchy mucus, a sustained BBT rise afterwards and a period around the expected time can help show whether ovulation likely occurred.
If the positive result happens close to your period, read it differently. It may reflect delayed ovulation, a late-cycle LH rise or pregnancy-test timing confusion. A late-cycle positive is discussed in more detail in the article on an LH surge before your period.

What a faint ovulation test line means with PCOS
A faint ovulation test line with PCOS usually means some LH is present, not that ovulation is about to happen. A line test is usually positive only when the test line is as dark as or darker than the control line, unless your test instructions say otherwise.
LH is normally present at low levels across the cycle. This means faint lines can appear even when you are not close to ovulation. With PCOS, faint or darker lines may appear more often, so the direction of change over several tests is more useful than one strip.
If the line is getting darker across several tests, continue tracking. If it never becomes clearly positive, you may have missed a short surge, tested too early or too late, used diluted urine, or had a cycle where ovulation did not occur.
When the line is unclear, compare it with your cycle day, mucus pattern and recent results. The article on a faint ovulation test line explains the difference between a visible line and a true positive result.
What if you get no positive ovulation test with PCOS?
No positive ovulation test with PCOS can mean the LH surge was missed, ovulation happened earlier or later than expected, urine was diluted, or the cycle did not ovulate. It does not prove, by itself, that you never ovulate.
Some LH surges are short and easy to miss with once-daily testing using LH test strips. Some cycles are longer than expected, which means testing may stop before the fertile window arrives. In other cycles, LH may rise in a way that a home test does not show clearly.
If you never see a positive across several cycles, add more context before assuming the result is final. Record cycle length, bleeding dates, cervical mucus, symptoms and BBT if you use it.
Several testing issues can cause unclear results, including testing too early, testing too late, using diluted urine or missing a short surge. These patterns are covered in the article on negative ovulation test results.
How cervical mucus helps when cycles are irregular
Cervical mucus can help when cycles are irregular because it reflects oestrogen changes before ovulation. Clear, wet, slippery or stretchy mucus can suggest the fertile window may be opening, but it cannot prove ovulation happened.
Some people with PCOS or PMOS notice fertile-looking mucus more than once in a cycle. This can happen when oestrogen rises, ovulation is delayed, or the body prepares for ovulation more than once.
If mucus becomes fertile-looking but your LH test stays negative, keep tracking for another day or two. A surge may still be coming, or the cycle may not ovulate. One confusing cycle is common, but repeated unclear cycles should be discussed with your GP.
Mucus is most useful when it is treated as one part of the picture. If you notice egg-white mucus but no matching LH rise or temperature shift, the article on fertile cervical mucus without ovulation explains why this can happen.
How BBT can help confirm ovulation with PCOS
BBT can help confirm ovulation with PCOS after the fertile window has passed. LH tests and mucus suggest ovulation may be approaching, while a sustained temperature rise can support that ovulation likely happened afterwards.
Basal body temperature is taken first thing after waking, before getting out of bed or moving around much. A single temperature does not tell you much. The pattern across several days is more useful.
With PCOS or PMOS, BBT charts can be harder to read if sleep is irregular, shift work is involved, illness occurs, or ovulation is delayed. This does not make BBT useless. It means BBT should be read with LH tests, mucus and cycle dates.
A temperature chart can add useful context, but it should not be used to diagnose pregnancy or a cycle problem. If you notice a second temperature rise later in the luteal phase, compare it with the article on triphasic chart patterns.
How to time sex when ovulation is irregular
When ovulation is irregular, timing sex works best when you respond to fertile signs rather than relying only on a predicted calendar date. A positive LH test, fertile mucus and recent cycle history can help narrow the fertile window.
If you see fertile mucus, consider starting or increasing LH testing. If your LH test becomes clearly positive around the same time, many people time sex that day and the following day.
If you have long cycles, you may need to keep the timing flexible. Trying to time sex every day across a long uncertain window can become stressful. A practical approach is to watch for fertile signs, then focus timing around those days.
A positive ovulation test is most useful when it appears around the fertile window. For a more detailed timing explanation, see when to have sex after an LH surge.
When to use a pregnancy test with PCOS and irregular cycles
Use a pregnancy test instead of an ovulation test when your period is due or late. Ovulation tests detect LH. Pregnancy tests detect hCG. A late positive ovulation test cannot reliably tell you whether you are pregnant.
This is especially relevant if you have PCOS or PMOS and cycles are irregular. A late period may mean ovulation happened later than expected, pregnancy has occurred, or the cycle is longer than usual.
If you test for pregnancy before your period is due and the result is negative, repeat the test in two to three days if your period has not arrived. Use first morning urine if testing early.
Pregnant with PCOS and irregular cycles can be harder to recognise early because ovulation may happen later than expected. Speak with your GP if pregnancy tests are positive, unclear or do not match your symptoms. Seek urgent care for severe one-sided pelvic pain, shoulder tip pain, fainting, dizziness, heavy bleeding or pain that does not settle.
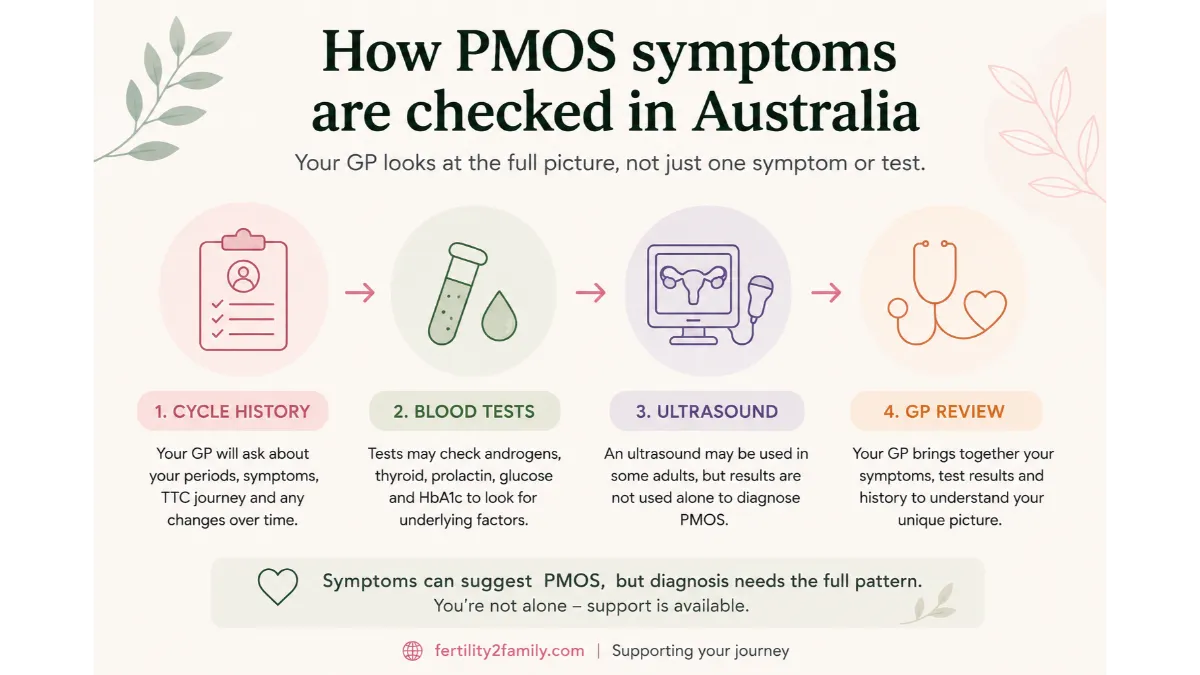
How ovulation is checked by a GP in Australia
In Australia, a GP can check ovulation by reviewing your cycle history, symptoms and tracking records, then arranging blood tests or ultrasound when needed. A mid-luteal progesterone blood test is often used when ovulation is uncertain.
For people with irregular cycles, progesterone timing should be matched to the expected period or suspected ovulation date, not automatically day 21. Your GP may also consider thyroid function, prolactin, androgen markers, metabolic screening and other tests depending on symptoms.
Ultrasound may be used to assess ovarian appearance, follicles, uterine factors or other causes of irregular cycles. It should be interpreted with symptoms and blood test results, because ultrasound alone does not explain every ovulation pattern.
Bring your GP a simple record of cycle dates, bleeding, LH results, mucus, BBT if used, medicines and symptoms. This is often more useful than a single screenshot of one ovulation test.
When to seek fertility review with PCOS or PMOS
Seek fertility review earlier if you have PCOS or PMOS and cycles are irregular, very long, absent or hard to track. Standard timing is 12 months of trying if under 35, or six months if 35 or older.
Earlier review is reasonable if you rarely bleed, have very unpredictable cycles, never see a clear ovulation pattern, have a known reproductive health condition, or have symptoms such as pelvic pain, heavy bleeding or repeated pregnancy loss.
Your GP may arrange initial investigations or refer you to a fertility specialist. This does not mean you cannot conceive naturally. It means you may need clearer information about ovulation, cycle timing and any other factors affecting fertility.
If PCOS or PMOS has been diagnosed, treatment options should be individualised. Lifestyle advice, medicines, ovulation induction, metabolic care and fertility referral all depend on symptoms, age, goals and medical history.
Frequently asked questions about tracking ovulation with PCOS Australia
Can PCOS cause positive ovulation tests without ovulation?
Yes. Some people with PCOS may see repeated positive or near-positive ovulation tests without clear ovulation. This can happen when baseline LH is higher, ovulation is delayed or a cycle does not ovulate. BBT, mucus patterns and GP-arranged progesterone testing can add context.
Can PCOS cause a false positive ovulation test?
Yes, it can. A false positive ovulation test with PCOS can happen when LH is high but ovulation does not follow. A single positive test is not enough to confirm ovulation. Look for the wider pattern, including mucus, BBT and cycle timing.
What if I never get a positive ovulation test with PCOS?
You may have missed a short surge, tested at the wrong time, diluted the urine, ovulated earlier or later than expected, or not ovulated that cycle. Track for more than one cycle and speak with your GP if positives remain absent or cycles are irregular.
Is BBT better than ovulation tests for PCOS?
BBT is not better for everyone. It answers a different question. Ovulation tests can suggest ovulation may be approaching, while BBT can support that ovulation likely happened afterwards. With PCOS, combining both methods can be more useful than relying on one sign.
Can inositol make ovulation easier to track?
Inositol may help some people with PCOS or PMOS, but it is not a guaranteed ovulation treatment and should not replace medical advice. Dose, timing and safety are covered separately in the article on inositol for PCOS and PMOS.
Should I see a GP before 12 months if I have PCOS?
Yes, earlier GP review is reasonable if cycles are irregular, absent, very long or hard to track. You do not need to wait 12 months if there are signs ovulation may be irregular. If you are 35 or older, seek advice after six months of trying.
Last reviewed: May 2026
Next scheduled review: May 2027
References
Fertility2Family publishes Australia-focused fertility education. Articles are written by our team and medically reviewed by Australian-registered health practitioners. We use Australian consumer medicine information, Australian clinical and public health guidance, and peer-reviewed research consistent with Australian care. We explain what the evidence suggests, what it cannot confirm, and when to see a GP or fertility specialist. Each article lists its author, medical reviewer, and review dates.
Better Health Channel. Ovulation and fertility. https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/ovulation
Healthdirect Australia. Polycystic ovarian syndrome. https://www.healthdirect.gov.au/polycystic-ovarian-syndrome-pcos
Healthdirect Australia. Fertility awareness. https://www.healthdirect.gov.au/fertility-awareness-natural-family-planning
Jean Hailes for Women’s Health. Polycystic ovary syndrome. https://www.jeanhailes.org.au/health-topics/pcos/
Jean Hailes for Women’s Health. How does PCOS affect fertility and pregnancy? https://www.jeanhailes.org.au/health-topics/pcos/how-does-pcos-affect-fertility-and-pregnancy/
RACGP. Assessment of female fertility in the general practice setting. https://www1.racgp.org.au/ajgp/2020/june/female-fertility-in-general-practice-setting
RACGP. An update on fertility assistance and assisted reproduction. https://www1.racgp.org.au/ajgp/2023/january-february/an-update-on-fertility-assistance-and-assisted-rep
Monash University. Polyendocrine Metabolic Ovarian Syndrome: New name to improve diagnosis and care. https://www.monash.edu/news/articles/polyendocrine-metabolic-ovarian-syndrome-new-name-to-improve-diagnosis-and-care-of-condition-affecting-170-million-women-worldwide
RANZCOG. RANZCOG welcomes PCOS renaming to PMOS. https://ranzcog.edu.au/news/ranzcog-welcomes-polycystic-ovarian-syndrome-pcos-renaming-to-polyendocrine-metabolic-ovarian-syndrome-pmos/
The Lancet. Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00717-8/fulltext
Human Reproduction Update. The LH surge and ovulation re-visited: a systematic review and meta-analysis. https://academic.oup.com/humupd/article-abstract/28/5/717/6544113