
13 min read
Dec 4, 2025
No LH Surge? What happens if you don’t have an LH surge?
Written by
Fertility2Family Team

Medically reviewed by
Evan Kurzyp, RN (AHPRA), BSN, Master of Nursing
Ovulation predictor kits help many Australians time sex for pregnancy or avoid sex when fertile. These small strips detect a sharp rise in luteinising hormone, often called the LH surge, which triggers the release of an egg about 24 to 36 hours later. Sometimes a kit never turns positive even when you expected to ovulate. That can be confusing and stressful. The good news is that most missed surges come down to timing, diluted urine, a short spike, or an irregular cycle rather than a serious problem. This guide explains how LH works, why OPKs can miss the surge, how to test well, what else to track at home, and when to see a GP or fertility specialist in Australia. It also shows how pregnancy and ovulation tests fit into a clear plan without overpromising results.
Quick Answers About LH Surge and Ovulation
Can you ovulate without an LH surge?
Physiology says ovulation needs an LH surge. You can conceive only if that surge occurs. What sometimes happens is the kit fails to detect the surge because it was short, you tested at the wrong time, your urine was too diluted, or your baseline LH is atypical.
Why is my OPK always negative?
Common causes include testing too early or late, a brief surge that you miss, dilute urine, an anovulatory cycle, or conditions like polycystic ovarian syndrome that change baseline LH. Cycle tracking and twice daily testing across your expected fertile window reduce the chance of a missed surge.
When should I use an OPK?
Start a few days before you expect to be fertile and test twice a day, morning and evening. Limit fluids for a couple of hours before testing. Keep going until you see a rise or your period arrives. Consistent timing improves accuracy.
What the LH Surge Is and How OPKs Work
Luteinising hormone is a reproductive hormone that regulates the menstrual cycle and triggers ovulation. You can read more about luteinising hormone at this overview. As the dominant follicle matures, oestrogen rises, then signals the brain to release a surge of LH. That surge triggers the final steps that release an egg from the ovary. For a clear introduction to ovulation, see this Victorian resource on ovulation.
Ovulation predictor kits measure LH in urine against a set threshold. Many kits register positive when LH reaches about 25 mIU/mL, a level that often precedes ovulation by about 24 to 36 hours. Some digital trackers can display a curve. Strips show a test line that must be as dark as or darker than the control line to be considered positive. A faint line is usually negative.
OPKs help you time sex if you want to conceive and help you avoid sex or use condoms during fertile days if you do not want pregnancy. They work best when you understand your cycle length and start testing a few days before you expect to be fertile. Timing matters far more than the brand you choose. You can learn more about identifying LH patterns in this guide to LH surge and timing intercourse.
LH surge: How to identify and use LH levels for pregnancy
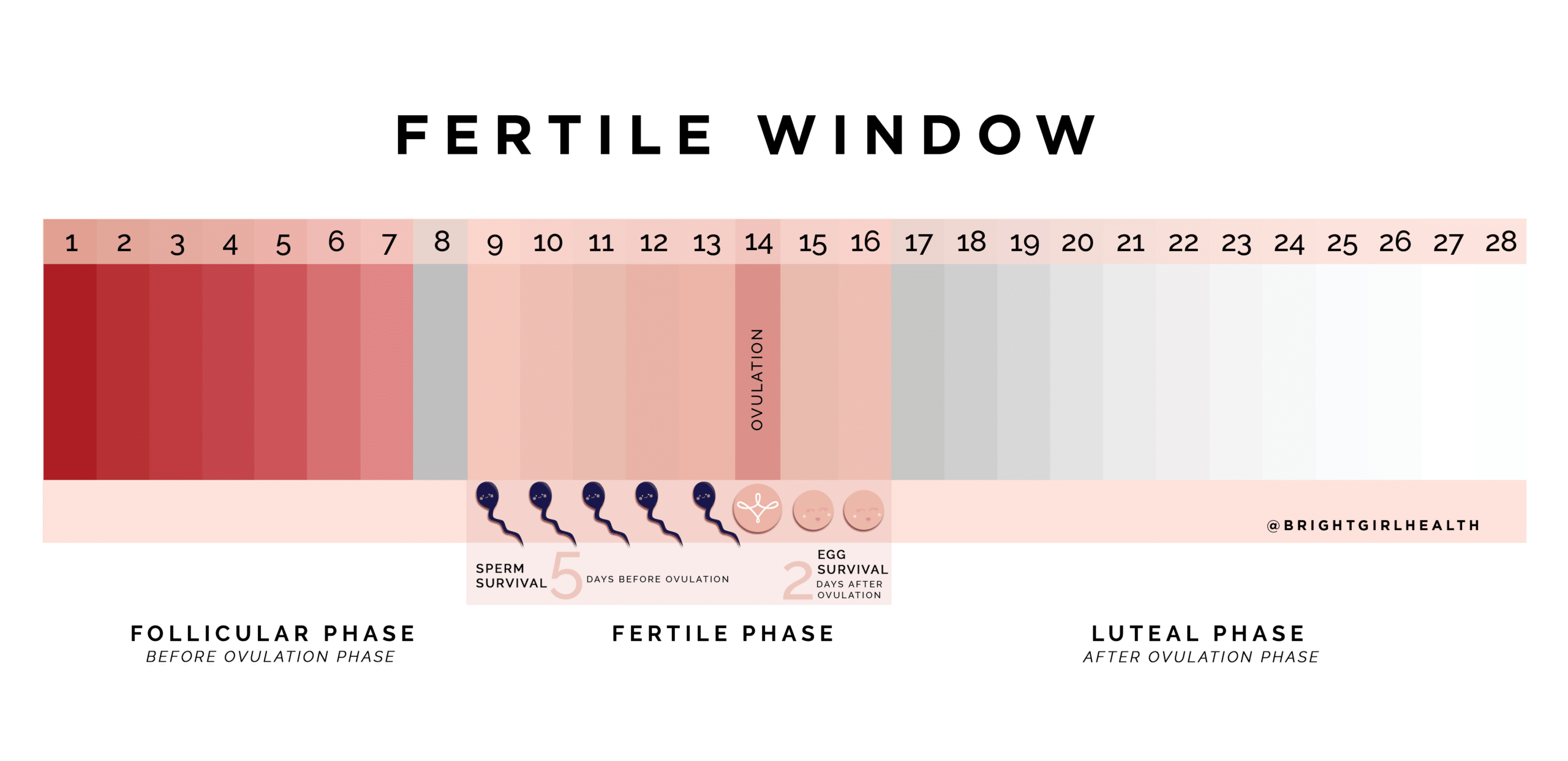 Image courtesy of The Bright Girl Guide by Demi Spaccavento
Image courtesy of The Bright Girl Guide by Demi Spaccavento
Causes of a Missing or Hard-to-Detect LH Surge
A negative OPK often means you have not yet reached the surge. If you expected a positive, think first about timing. You may have started too early or tested after the surge ended. Some people have a brief surge that lasts only part of a day, which is easy to miss with once daily testing.
Urine concentration affects results. Drinking a lot of water can dilute LH. Try limiting fluids for two hours before testing and hold urine for at least two to three hours. If you only test in the evening, consider adding a morning test during your fertile window to widen your chance of catching a short spike.
Baseline LH varies from person to person. A study of urinary hormones found LH 24 hours before ovulation could range from about 6.5 mIU/mL to over 100 mIU/mL. You can see a summary in this urinary hormone ranges report. If your baseline is low, a strip may not reach its positive threshold even if you ovulate. If your baseline is high, you may see more days that look close to positive, which can confuse timing.
Polycystic ovarian syndrome can raise baseline LH and make results difficult to interpret. Read about PCOS and hormones at Jean Hailes. Some cycles are anovulatory, which means you do not release an egg. An anovulatory cycle often presents with irregular or absent periods, spotting, or a cycle that varies widely in length. Learn about anovulatory cycles at this plain-language explainer.
Stress, illness, travel, sleep loss, and weight change can disrupt the hypothalamic pituitary ovarian axis. High cortisol can blunt the LH surge or delay it. Thyroid or prolactin issues can also shift or prevent ovulation. If you are using medicines that affect ovulation, such as letrozole or clomiphene, discuss test timing with your clinician, as the pattern can look different in medicated cycles. Some people ovulate later than expected. Read more on late ovulation.
How Ovulation Is Assessed in Australia
If your home results are unclear, your GP can review your cycle history, medical background, and medications. In Australia, initial testing usually includes a progesterone blood test about seven days before your expected period to confirm that ovulation occurred. Some GPs repeat the test if your cycles are irregular, as timing can be tricky.
Other tests can include thyroid function, prolactin, folate and vitamin D status, and sometimes anti-Müllerian hormone to consider ovarian reserve in context. If cycles are irregular or absent, your GP may order pelvic ultrasound to assess ovaries and track follicle development. You can read about LH blood testing principles in this LH blood test explainer, then discuss local protocols with your GP.
When pregnancy has not occurred after 12 months of regular unprotected sex under age 35, or after six months if you are 35 or older, the usual pathway is a GP review and possible referral to a fertility specialist. If you have known factors such as very irregular periods, prior pelvic surgery, severe period pain, or suspected endometriosis, referral can happen earlier. Australian guidance through Healthdirect, RACGP, and RANZCOG supports timely assessment to avoid long delays in care.
What Ovulation Tests Involve and How to Use Them Well
An OPK measures LH in urine. Strips, cassettes, and in-stream sticks work similarly. Read the instructions and store tests in a cool, dry place. Begin testing a few days before you expect your fertile window. If your cycles are variable, start earlier and keep going until your period starts or you see a clear positive.
Collect urine in a clean cup if using strip tests. Dip the strip to the marked line for the time specified in the instructions and lay it flat. Read within the time window. For in-stream tests, hold the absorbent tip in the urine stream for the recommended seconds, then place it flat and read on time. A positive is when the test line is the same colour or darker than the control line. Digital devices display a symbol when the threshold is reached, which can be easier to read but relies on internal cut-offs that still vary by person.
Test twice daily in your fertile window to reduce the chance of missing a brief surge. Limit fluids beforehand. If your lines are often almost positive, note that some conditions such as PCOS can raise baseline LH. In those cases, do not rely on OPKs alone. Combine methods and consider clinical advice if you are unsure.
 How to read in-stream ovulation test kit results
How to read in-stream ovulation test kit results
Home Management: Tracking Signs, Temperature and Cervical Mucus
At home, combine OPKs with body signs to build a clearer picture. Cervical mucus often shifts from creamy to clear, stretchy fluid like raw egg white as ovulation approaches. This change increases sperm movement and survival. You can read about cervical mucus patterns at Jean Hailes. Basal body temperature, measured first thing each morning with a sensitive thermometer, usually rises slightly after ovulation due to progesterone. This confirms that ovulation has happened and helps you understand your individual timing across cycles. Learn more at this explainer.
Some people notice a brief one-sided lower tummy ache around mid cycle called mittelschmerz, which can line up with ovulation. Others notice higher libido, mild breast tenderness, or subtle mood and energy changes around fertile days. These signs are helpful context. They are not proof on their own, so use them alongside tests and temperature tracking.
Nutrition, sleep, and daily routine affect hormones. Regular meals with balanced protein, fibre, and healthy fats support stable blood glucose and help the brain ovary signalling that drives ovulation. A consistent sleep schedule supports circadian timing of hormone release. If you drink alcohol, keep intake low when trying to conceive. Avoid smoking. Aim for regular movement and a weight range that fits your health plan. Discuss any supplements or herbal products with your GP before starting them.
 Am I ovulating? Physical signs that you are fertile
Am I ovulating? Physical signs that you are fertile
When to See a GP or Fertility Specialist in Australia
Seek care if you have cycles shorter than 21 days or longer than 35 days, if your period has stopped for three months when not pregnant, or if you have very heavy bleeding, severe pelvic pain, or fever. These can point to conditions that need assessment. If you keep missing an LH rise after two or three cycles of careful twice daily testing, book a GP appointment. Bring your cycle dates, OPK photos, and any temperature or mucus records. That information helps your GP decide on blood tests or ultrasound.
Make an appointment sooner if you have signs of thyroid problems, milk discharge unrelated to breastfeeding, acne and hair growth that is new or worsening, or a known history of endometriosis or pelvic inflammatory disease. If you are 35 or older and have tried for six months without success, discuss referral early. If your partner has known fertility concerns, arrange a semen analysis through your GP. Early review can reduce uncertainty and help you plan next steps without losing time.
Where Ovulation and Pregnancy Tests Fit Into Your Fertility Plan
OPKs tell you when the fertile window is opening. Pregnancy tests detect human chorionic gonadotrophin, or hCG, after implantation. Used together with cycle knowledge, they help you act at the right time and avoid long periods of guesswork. If you think you missed your surge on strips, adding a digital device for one to two cycles can help you compare thresholds. You can also run a strip and a digital test on the same urine sample to learn how your pattern looks across brands and formats.
Use pregnancy tests from the day your period is due for the best balance of accuracy and reassurance. Early testing is possible, though a negative before your period is due can change to a positive after a couple of days. Exposure to heat or moisture can damage test accuracy, so store all kits as directed.
If you want to compare formats, you can find strip, cassette, and in-stream options here: ovulation tests. To test regularly for a full cycle and learn your pattern, this bulk option can help with daily use: ovulation test and collection cups. If you are timing sex, this guide to how often to have sex explains practical options. For context on LH thresholds and test accuracy, this overview of how accurate LH ovulation tests are can help.
 How accurate are LH ovulation tests?
How accurate are LH ovulation tests?
Frequently Asked Questions About LH Surge and Ovulation Australia
Is a faint line on an OPK positive?
A faint test line is usually negative because the LH level has not reached the positive threshold. The test line must match or exceed the control line in colour to be positive. Keep testing across your expected fertile days to catch the rise.
Should I use first morning urine for OPKs?
First morning urine can work for some people but often gives misleading results due to overnight concentration. Many find late morning or early evening best. Aim for two to three hours without urinating and avoid excess fluids before testing for more consistent results.
Can stress stop the LH surge?
High and persistent stress can delay or blunt the LH surge by affecting brain signals that regulate the ovaries. Good sleep, regular meals, movement, and practical stress supports can help. If cycles remain irregular, see your GP for a review.
Why do I get several days of high readings?
Some people have a gradual rise, especially with digital readers that show high fertility before peak. Others have a high baseline LH, which is more common in PCOS. Look for a clear shift to your strongest reading and confirm with temperature tracking if possible.
How soon after a positive OPK should we have sex?
Sperm live in the reproductive tract for several days. Sex on the day of your first positive and the following day covers the highest chance window. If you are testing twice daily, consider sex on the evening of the first positive and the next day.
Do supplements boost the LH surge?
There is no single supplement that reliably increases LH in healthy cycles. Focus on overall health, a balanced diet, and routine. If you have a diagnosed deficiency such as iodine or vitamin D, follow your GP’s advice. Avoid self-prescribing high dose products without guidance.
Next Steps If You Keep Missing the LH Surge
If your OPK has not shown a clear surge after two or three cycles of careful timing and twice daily testing, do not blame yourself or the products too quickly. Book a GP appointment and bring your records. Your doctor can check thyroid, prolactin, and ovulation blood tests, and consider pelvic ultrasound if cycles are irregular. If everything looks normal, a simple plan that combines OPKs, basal temperature, and cervical mucus tracking across another cycle often fills in the gaps, especially if your natural surge is brief.
If results point to a condition such as PCOS, thyroid disorder, or hyperprolactinaemia, early treatment can improve cycles and support your fertility goals. If you are ready to keep tracking at home, you can test daily for one full cycle to learn your personal pattern using a mix of strip and in-stream tests. If you prefer guidance, speak with your GP about local fertility clinics, RANZCOG specialists, or state family planning services. With the right plan, you can reduce uncertainty and move forward with more confidence.
References
https://www.healthdirect.gov.au/ovulation
https://www.healthdirect.gov.au/infertility
https://www.ranzcog.edu.au/womens-health/patient-information-resources/ovulation-and-fertility
https://www.jeanhailes.org.au/health-a-z/periods/menstrual-cycle
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/ovulation
https://www.fpnsw.org.au/health-information/sex-and-fertility/fertility
https://www.qld.gov.au/health/staying-healthy/sexual-health/fertility
https://www.health.nsw.gov.au/kidsfamilies/MCFhealth/Pages/fertility.aspx


