11 min read
Dec 1, 2025
Can I Have Fertile Cervical Mucus and Not Ovulate?
Written by
Fertility2Family Team

Medically reviewed by
Evan Kurzyp, RN (AHPRA), BSN, Master of Nursing
If you are trying to conceive, you are likely watching two things most closely: fertile cervical mucus and a rise in basal body temperature. Egg white cervical mucus often appears in the days before ovulation and helps sperm travel. A temperature shift usually follows ovulation as progesterone rises. Some cycles are not so clear. You might see slippery, stretchy mucus but your temperature chart looks flat or messy. This does not always mean you did not ovulate, but it does make timing trickier. This guide explains how cervical mucus, luteinising hormone and temperature fit together, why patterns sometimes clash, how ovulation is confirmed in Australia, and when to talk with your GP. It also shows how at‑home tools can support your tracking without making promises they cannot keep.
Quick Answers About Cervical Mucus, Temperature and Ovulation
How long after egg white cervical mucus do you ovulate?
Egg white cervical mucus often appears in the lead‑up to ovulation. Many people ovulate within one to three days of their most slippery mucus, but timing varies by cycle.
Does a temperature rise always confirm ovulation?
A sustained rise in basal body temperature usually follows ovulation, driven by progesterone. Some charts are noisy due to sleep, illness or shift work, so a clear rise may be hard to see.
Can you have fertile mucus without ovulating?
Yes. Oestrogen can rise and create fertile mucus without an egg being released. Conditions like PCOS, stress, breastfeeding or perimenopause can cause this pattern.
What Cervical Mucus Is And What It Tells You
Cervical mucus is made by glands in the cervix. Its job changes across the cycle. When oestrogen rises in the follicular phase, mucus becomes thin, wet and stretchy. This texture helps sperm move through the cervix and survive in the reproductive tract. When progesterone rises after ovulation, mucus thickens and becomes tacky or creamy. This forms a barrier that is less friendly to sperm. Many people describe their most fertile mucus as clear and stretchy like raw egg white. This is a useful sign that your body is preparing to release an egg, but it is not proof that ovulation has happened.
Some people choose to learn their own mucus pattern across several cycles. You can read more about typical changes and what to look for in our guide to cervical mucus and how it relates to the menstrual cycle. Others prefer a mixed approach that combines mucus, ovulation testing and temperature for a clearer picture.
Why Fertile Mucus Can Appear Without a Temperature Rise
Cervical mucus reflects oestrogen. Basal body temperature reflects progesterone. They are different hormones with different timing. You may see several days of fertile mucus, then ovulate, and only notice a temperature rise after the egg is released. If the chart is noisy, that rise can be small or unclear.
There are also cycles where oestrogen rises and produces fertile mucus but ovulation does not occur. This is called an anovulatory cycle. Some people see this occasionally and still conceive later. Frequent anovulatory cycles can point to conditions such as polycystic ovary syndrome, thyroid disorders or hypothalamic amenorrhoea. Breastfeeding, stopping hormonal contraception, recent illness and perimenopause can create patches of fertile mucus without a clear ovulation pattern. Medications, stress, poor sleep and alcohol can flatten or distort temperature charts. Mouth breathing or taking your temperature at different times can also blur the shift.
If you are unsure whether you ovulated in a given cycle, an integrated approach that pairs mucus with urine luteinising hormone testing adds more clarity.
How Ovulation Is Diagnosed And Confirmed In Australia
In everyday tracking, ovulation is suggested by a positive luteinising hormone test and a sustained basal temperature rise. In clinical settings, ovulation can be confirmed through blood tests and ultrasound. A GP may order a serum progesterone test in the mid luteal phase, usually about seven days after suspected ovulation, to check whether levels rose as expected. Your GP may also arrange a pelvic ultrasound. An ultrasound before ovulation can show a growing follicle. A follow‑up can show that the follicle has collapsed and that a corpus luteum has formed, both signs that an egg likely released.
Australian pathways commonly start with a GP review that includes menstrual history, medication review, screening for thyroid and prolactin levels, and a discussion of timing and lifestyle. If cycles are irregular or you have been trying for a year under 35, or six months if 35 or older, your GP may refer you to a fertility specialist. The specialist can organise further tests or treatment that match your medical history and goals.
What The Tests Involve: LH, Temperature, Bloods And Ultrasound
Luteinising hormone testing uses a urine strip to detect the surge that triggers ovulation. Most people will ovulate about 24 to 36 hours after the LH peak. Testing twice daily around your fertile window can help you catch a short surge. Ovulation tests can be useful if your mucus is confusing or you want an extra signal to time intercourse.
Basal body temperature requires a reliable thermometer and a consistent routine. Take your temperature first thing after waking, before getting out of bed or talking. Try to measure at the same time each day after several hours of sleep. A basal body thermometer with two decimal places can make trends easier to read. The rise often appears across two or three readings and stays higher until your next period.
Blood tests check hormones that affect ovulation. Your GP may check thyroid function and prolactin. A mid luteal progesterone test helps confirm that ovulation occurred. Ultrasound can track follicle growth and the presence of a corpus luteum. In some cases, your doctor may also assess for ovarian cysts and uterine factors if symptoms suggest a problem. If you do not ovulate regularly, your specialist may discuss medication to induce ovulation where appropriate.

Home Management: Using Mucus, LH And Temperature Together
You do not need to track every small change. Focus on daily mucus pattern, a short period of LH testing near your expected fertile days, and a consistent temperature routine. Start by noting the first day you see wetter mucus after your period. If you prefer, begin testing with ovulation tests once mucus becomes watery or stretchy. When you record a positive LH, plan intercourse over the next day or two. Keep taking your temperature each morning. A sustained rise supports that ovulation has likely occurred.
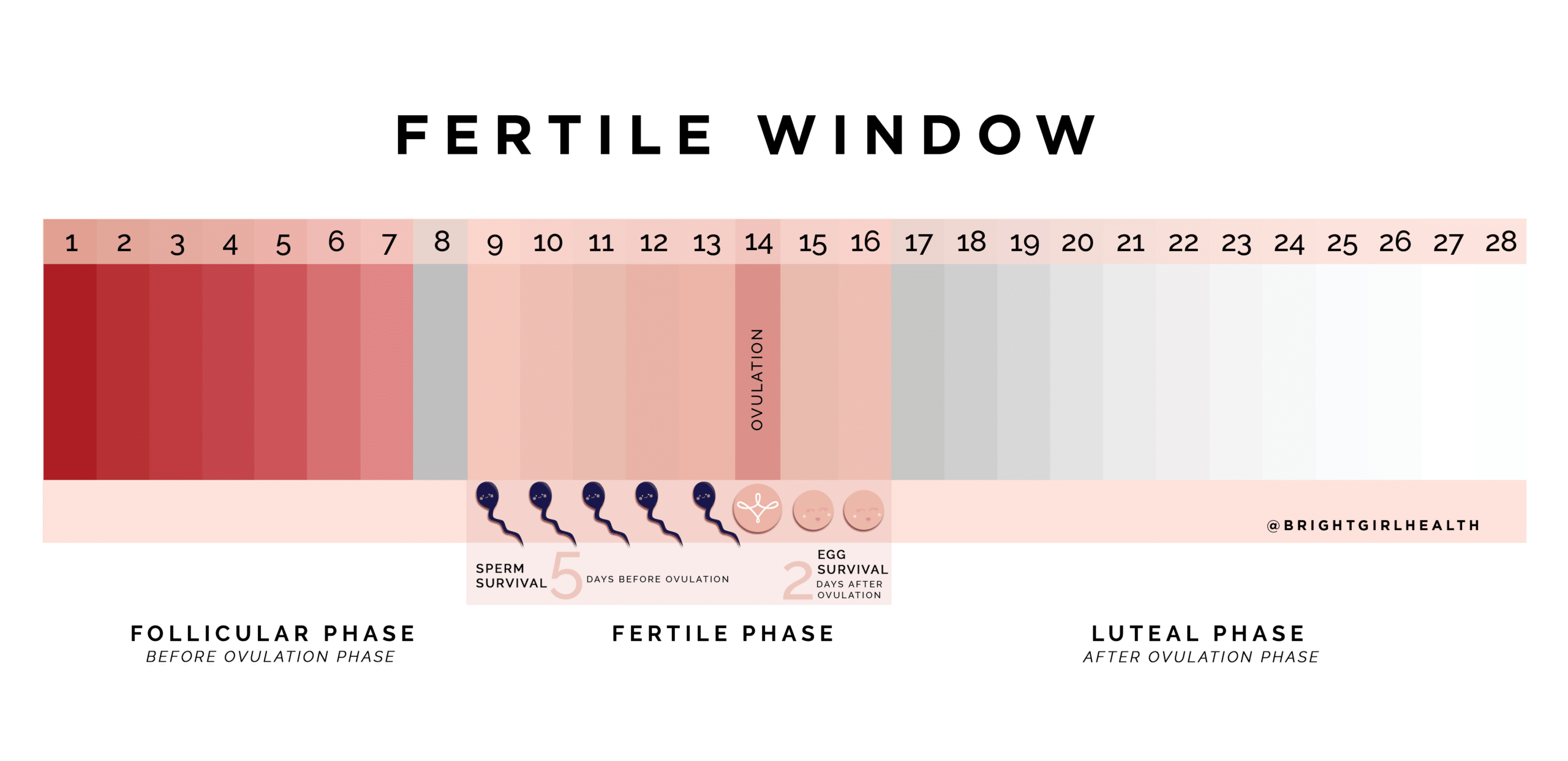
If mucus is present but LH tests do not turn positive, you may be seeing an oestrogen rise without an LH surge. This can still be a good time to try, as sperm can live in fertile mucus for up to five days. If your temperature does not climb in the week after your mucus peak and LH testing remained negative, ovulation may not have happened. One unclear cycle is common. If this repeats, talk with your GP. Tracking across several cycles usually reveals a pattern that suits your body and routine.
Why A Temperature Rise Might Be Hard To See
Temperature charts depend on steady conditions. Short sleep, waking at different times, alcohol, fever, and shift work can all flatten the rise. Mouth breathing or taking your temperature after getting up can also affect readings. Some people simply have a small progesterone‑related rise that sits within normal day to day variation. This does not mean ovulation failed. It only means temperature is not the clearest tool for you on its own.
If you often miss the rise, adjust what you can. Keep your room and routine as consistent as possible. Avoid alcohol late in the evening during the fertile window. Use the same thermometer every day. Pair temperature with mucus and LH testing so that one method backs up the others. If charts remain unclear and you are not conceiving, ask your GP about blood tests to check progesterone about seven days after suspected ovulation.
When To See A GP Or Specialist In Australia
See your GP if your cycles are longer than 35 days, shorter than 21 days, or vary widely from month to month. Seek advice if you have frequent spotting, very heavy bleeding, severe pain, or symptoms of hormonal imbalance such as new acne or excess hair growth. If you are under 35 and have been trying for 12 months, or 35 or older and have been trying for six months, book a review. If you suspect you are not ovulating regularly, ask about a plan to confirm this and possible next steps.
Your GP may order hormone tests, an ultrasound and a semen analysis for your partner. They may discuss weight, nutrition, sleep and exercise. Many people conceive with lifestyle changes and better timing. If needed, your GP can refer you to a fertility specialist who can consider ovulation induction medication, further tests or assisted reproductive options where appropriate. Care should match your goals and medical history.
How Fertility2Family Products Fit Into Your Tracking
At‑home tools can make cycle tracking more practical. Ovulation tests detect the LH surge that triggers ovulation and can refine your timing when mucus is confusing or you are unsure of your cycle day. A basal body thermometer helps you spot a temperature shift after ovulation to confirm your fertile window has passed. Fertility kits combine tests and collection cups for convenience and consistency. Once you are in the luteal phase, pregnancy tests can be used from the day of your expected period, or a little earlier with the understanding that very early testing may be negative even if you are pregnant.
These tools do not diagnose medical conditions and they cannot promise ovulation or pregnancy. They are best used alongside knowledge of your own cycle signs. If you are unsure about your results or your cycle pattern, use them as conversation starters with your GP or fertility nurse. Good records help your clinician give tailored advice that suits Australian care pathways.
Frequently Asked Questions About Cervical Mucus, Temperature and Ovulation Australia
Can egg white cervical mucus appear more than once in a cycle
Yes. You might see a patch of fertile mucus that fades, then returns before you ovulate. This often happens after illness, stress or when cycles are resetting after stopping contraception.
How soon after a positive LH test should we try
Most people ovulate within 24 to 36 hours of a positive test. Many couples time intercourse on the day of the positive and the day after for coverage.
Is creamy or sticky mucus fertile
Creamy or sticky mucus usually appears outside the fertile window. Watery or stretchy mucus is more associated with higher fertility, but patterns vary by person.
Do pain or twinges prove ovulation
Some feel mid‑cycle discomfort around ovulation. This can be a helpful sign, but it is not proof. Pair body signals with LH testing or a temperature rise for better confidence.
What if my progesterone blood test is low
A single low reading can miss the timing. Your GP may repeat the test or arrange ultrasound tracking. If ovulation is irregular, your doctor may discuss treatment where suitable.
Does coffee or alcohol affect fertility tracking
Alcohol can disturb sleep and blunt temperature patterns. Coffee may shift your wake time. Aim for consistent sleep and test conditions in the fertile window where possible.
Final Thoughts And Next Steps For Your Fertile Window
Fertile cervical mucus is a helpful sign that sperm have the best chance to survive and reach an egg. A temperature rise shows what has already happened rather than what will happen. Using both signs together, and adding LH testing when needed, gives you practical coverage of your fertile days without second‑guessing. If you are seeing fertile mucus without a clear temperature rise, adjust what you can control. Keep wake times steady, avoid late alcohol in your fertile week, and use the same thermometer every day. Test LH around the time your mucus becomes slippery to catch a short surge. Record results for several cycles so patterns emerge. If your cycle remains irregular or you are not conceiving within the usual time frames, speak with your GP. Australian care pathways are set up to review your history, run the right tests, and step in when that will help. If you want simple tools to support your plan, Fertility2Family offers ovulation tests, basal body thermometers and pregnancy tests so you can track with confidence and talk with your clinician using clear, consistent records.
References
https://www.healthdirect.gov.au/fertility-awareness-natural-family-planning
https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/ovulation
https://www.racgp.org.au/afp/2012/march/infertility
https://ranzcog.edu.au/womens-health/patient-information-resources/understanding-fertility
https://www.jeanhailes.org.au/health-a-z/periods/fertility
https://www.health.qld.gov.au/news-events/news/fertility-pregnancy-trying-to-conceive
https://www.health.nsw.gov.au/kidsfamilies/MCFhealth/Pages/planning-pregnancy.aspx
https://ww2.health.wa.gov.au/Articles/F_I/Fertility-and-infertility